The Cost-Effectiveness of Birth-Cohort Screening for Hepatitis C Antibody in U.S. Primary Care Settings
Supporting Files

-
Nov 04 2011
-
File Language:
English
Details
-
Alternative Title:Ann Intern Med
-
Personal Author:
-
Description:Background
In the United States, hepatitis C virus (HCV) infection is most prevalent among adults born from 1945 through 1965, and approximately 50% to 75% of infected adults are unaware of their infection.
Objective
To estimate the cost-effectiveness of birth-cohort screening.
Design
Cost-effectiveness simulation.
Data Sources
National Health and Nutrition Examination Survey, U.S. Census, Medicare reimbursement schedule, and published sources.
Target Population
Adults born from 1945 through 1965 with 1 or more visits to a primary care provider annually.
Time Horizon
Lifetime.
Perspective
Societal, health care.
Intervention
One-time antibody test of 1945–1965 birth cohort.
Outcome Measures
Numbers of cases that were identified and treated and that achieved a sustained viral response; liver disease and death from HCV; medical and productivity costs; quality-adjusted life-years (QALYs); incremental cost-effectiveness ratio (ICER).
Results of Base-Case Analysis
Compared with the status quo, birth-cohort screening identified 808 580 additional cases of chronic HCV infection at a screening cost of $2874 per case identified. Assuming that birth-cohort screening was followed by pegylated interferon and ribavirin (PEG-IFN + R) for treated patients, screening increased QALYs by 348 800 and costs by $5.5 billion, for an ICER of $15 700 per QALY gained. Assuming that birth-cohort screening was followed by direct-acting antiviral plus PEG-IFN + R treatment for treated patients, screening increased QALYs by 532 200 and costs by $19.0 billion, for an ICER of $35 700 per QALY saved.
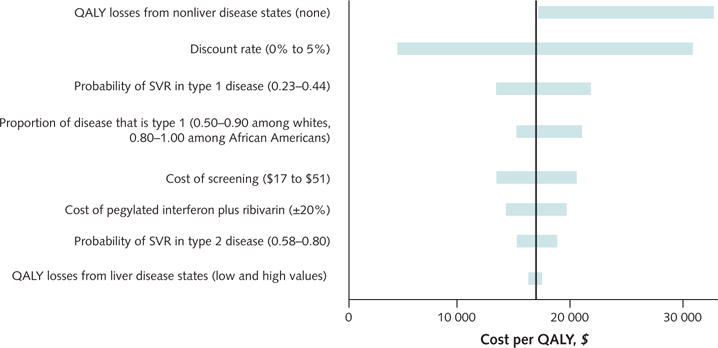
Results of Sensitivity Analysis
The ICER of birth-cohort screening was most sensitive to sustained viral response of antiviral therapy, the cost of therapy, the discount rate, and the QALY losses assigned to disease states.
Limitation
Empirical data on screening and direct-acting antiviral treatment in real-world clinical settings are scarce.
Conclusion
Birth-cohort screening for HCV in primary care settings was cost-effective.
Primary Funding Source
Division of Viral Hepatitis, Centers for Disease Control and Prevention.
-
Subjects:
-
Source:Ann Intern Med. 156(4):263-270.
-
Pubmed ID:22056542
-
Pubmed Central ID:PMC5484577
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:156
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:6183422539cbe158126f05a561a06b223add0efafdad4d30d367930685fd63b3
-
Download URL:
-
File Type:
 [PDF
- 164.33 KB
]
[PDF
- 164.33 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access