Assessing Effectiveness of Ceiling-Ventilated Mock Airborne Infection Isolation Room in Preventing Hospital-Acquired Influenza Transmission to Health Care Workers
Supporting Files

-
2016
Details
-
Alternative Title:ASHRAE Trans
-
Personal Author:
-
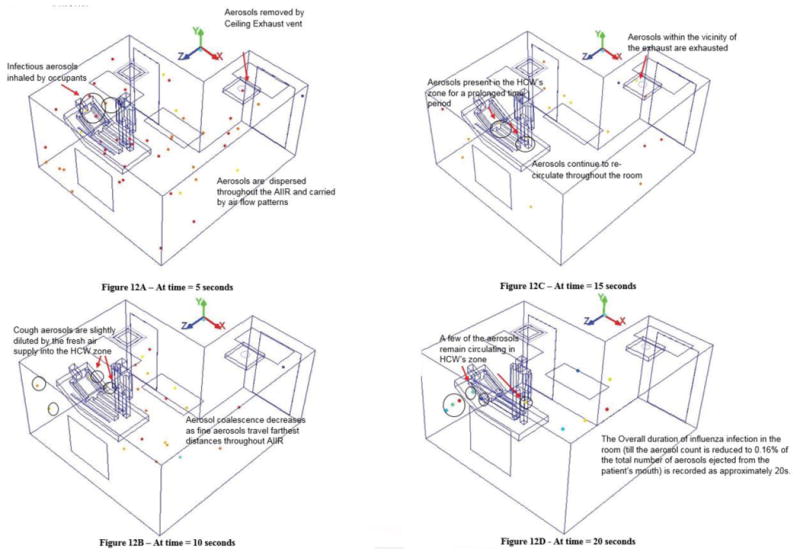
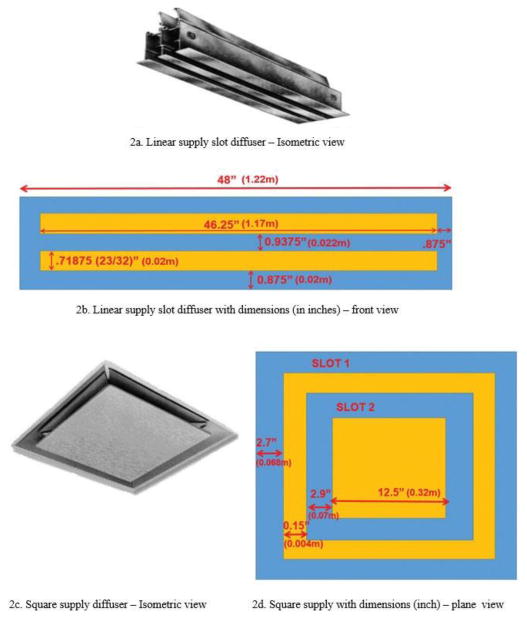
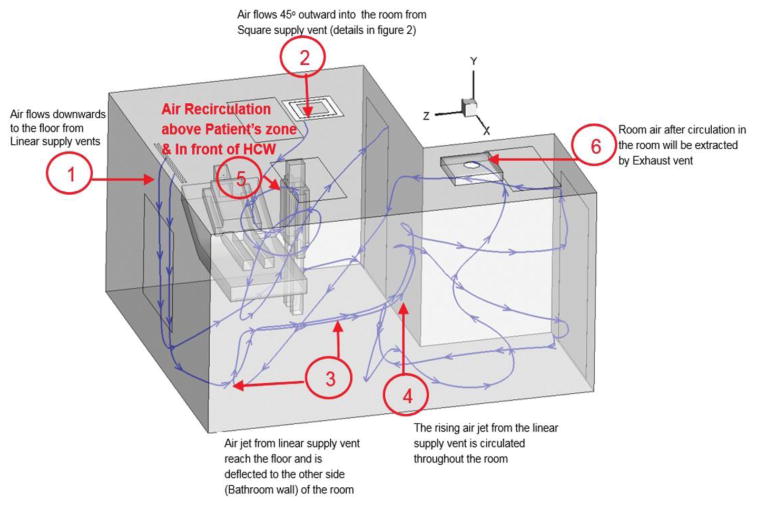
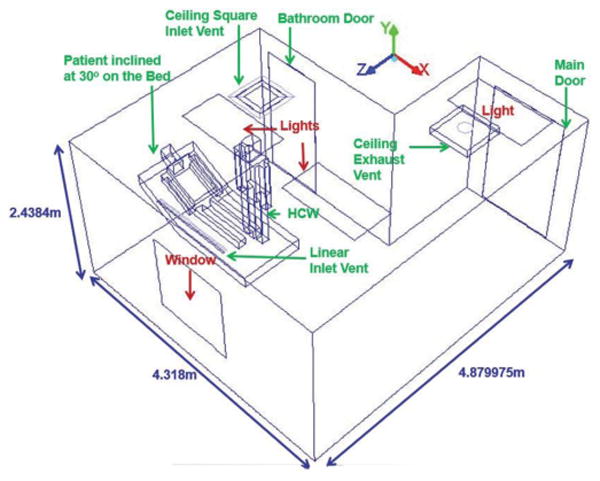
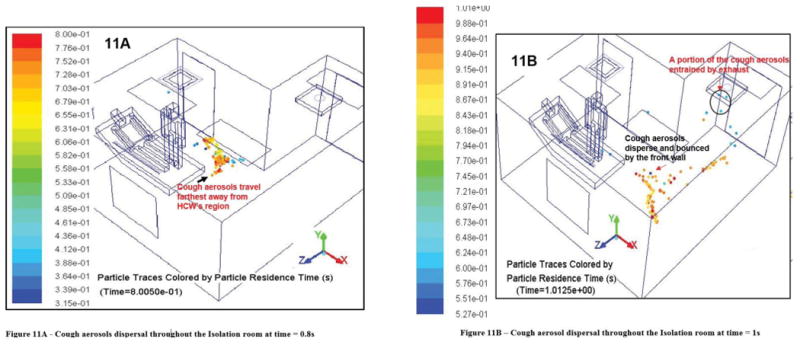
Description:Exposure to airborne influenza (or flu) from a patient's cough and exhaled air causes potential flu virus transmission to the persons located nearby. Hospital-acquired influenza is a major airborne disease that occurs to health care workers (HCW). This paper examines the airflow patterns and influenza-infected cough aerosol transport behavior in a ceiling-ventilated mock airborne infection isolation room (AIIR) and its effectiveness in mitigating HCW's exposure to airborne infection. The computational fluid dynamics (CFD) analysis of the airflow patterns and the flu virus dispersal behavior in a mock AIIR is conducted using the room geometries and layout (room dimensions, bathroom dimensions and details, placement of vents and furniture), ventilation parameters (flow rates at the inlet and outlet vents, diffuser design, thermal sources, etc.), and pressurization corresponding to that of a traditional ceiling-mounted ventilation arrangement observed in existing hospitals. The measured data shows that ventilation rates for the AIIR are about 12 air changes per hour(ach). However, the numerical results reveals incomplete air mixing and that not all of the room air is changed 12 times per hour. Two life-sized breathing human models are used to simulate a source patient and a receiving HCW. A patient cough cycle is introduced into the simulation and the airborne infection dispersal is tracked in time using a multiphase flow simulation approach. The results reveal air recirculation regions that diminished the effect of air filtration and prolong the presence of flu-contaminated air at the HCW's zone. Immediately after the patient coughs (0.51 s), the cough velocity from the patient's mouth drives the cough aerosols toward the HCW standing next to patient's bed. Within 0.7 s, the HCW is at risk of acquiring the infectious influenza disease, as a portion of these aerosols are inhaled by the HCW. As time progresses (5 s), the aerosols eventually spread throughout the entire room, as they are carried by the AIIR airflow patterns. Subsequently, a portion of these aerosols are removed by the exhaust ventilation. However, the remaining cough aerosols reenter and recirculate in the HCW's zone until they are removed by the exhaust ventilation. The infectious aerosols become diluted in the HCW's region over a period of 10 s because of the fresh air supplied into the HCW's zone. The overall duration of influenza infection in the room (until the aerosol count is reduced to less than 0.16% of the total number of aerosols ejected from the patient's mouth) is recorded as approximately 20 s. With successive coughing events, a near-continuous exposure would be possible. Hence, the ceiling-ventilation arrangement of the mock AIIR creats an unfavorable environment to the HCW throughout his stay in the room, and the modeled AIIR ventilation is not effective in protecting the HCW from infectious cough aerosols. The CFD results suggest that the AIIR ceiling ventilation arrangement has a significant role in influencing the flu virus transmission to the HCW.
-
Subjects:
-
Source:ASHRAE Trans. 122(2):35-46.
-
Pubmed ID:28529344
-
Pubmed Central ID:PMC5438175
-
Document Type:
-
Funding:
-
Volume:122
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha256:a05a6a93ae84a86918f70446b8fa96c0c396349a440deeb35cf99919fafdcab5
-
Download URL:
-
File Type:
 [PDF
- 975.92 KB
]
[PDF
- 975.92 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access