Evaluation of Rural vs Urban Trauma Patients Served by 9-1-1 Emergency Medical Services
Supporting Files

-
Jan 01 2017
-
File Language:
English
Details
-
Alternative Title:JAMA Surg
-
Personal Author:
-
Description:Importance
Despite a large rural US population, there are potential differences between rural and urban regions in the processes and outcomes following trauma.
Objectives
To describe and evaluate rural vs urban processes of care, injury severity, and mortality among injured patients served by 9-1-1 emergency medical services (EMS).
Design, Setting, and Participants
This was a preplanned secondary analysis of a prospective cohort enrolled from January 1 through December 31, 2011, and followed up through hospitalization. The study included 44 EMS agencies transporting to 28 hospitals in 2 rural and 5 urban counties in Oregon and Washington. A population-based, consecutive sample of 67047 injured children and adults served by EMS (1971 rural and 65 076 urban) was enrolled. Among the 53 487 patients transported by EMS, a stratified probability sample of 17 633 patients (1438 rural and 16 195 urban) was created to track hospital outcomes (78.9% with in-hospital follow-up). Data analysis was performed from June 12, 2015, to May 20, 2016.
Exposures
Rural was defined at the county level by 60 minutes or more driving proximity to the nearest level I or II trauma center and/or rural designation in the Centers for Medicare & Medicaid Services ambulance fee schedule by zip code.
Main outcomes and Measures
Mortality (out-of-hospital and in-hospital), need for early critical resources, and transfer rates.
Results
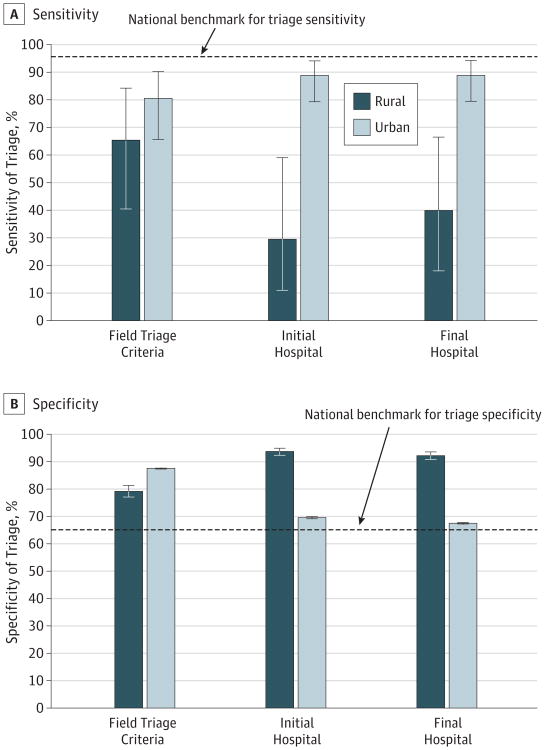
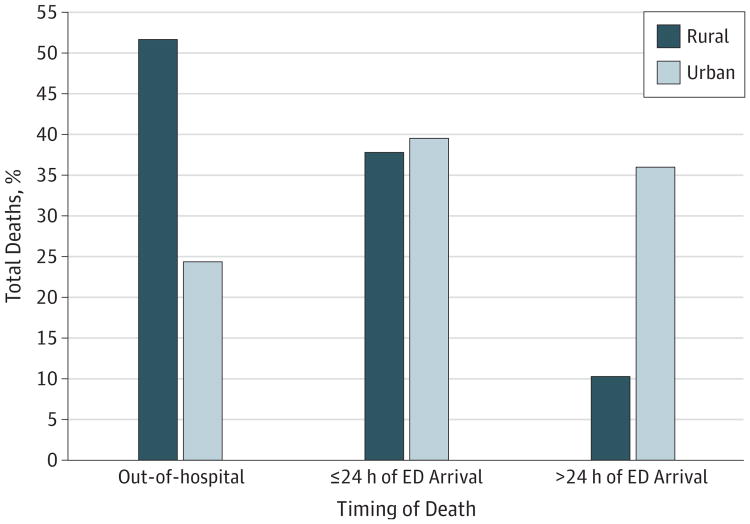
Of the 53 487 injured patients transported by EMS (17 633 patients in the probability sample), 27 535 were women (51.5%); mean (SD) age was 51.6 (26.1) years. Rural vs urban sensitivity of field triage for identifying patients requiring early critical resources was 65.2% vs 80.5%, and only 29.4% of rural patients needing critical resources were initially transported to major trauma centers vs 88.7% of urban patients. After accounting for transfers, 39.8% of rural patients requiring critical resources were cared for in major trauma centers vs 88.7% of urban patients. Overall mortality did not differ between rural and urban regions (1.44% vs 0.89%; P = .09); however, 89.6% of rural deaths occurred within 24 hours compared with 64% of urban deaths. Rural regions had higher transfer rates (3.2% vs 2.7%) and longer transfer distances (median, 97.4 km; interquartile range [IQR], 51.7-394.5 km; range, 47.8-398.6 km vs 22.5 km; IQR, 11.6-24.6 km; range, 3.5-97.4 km).
Conclusions and Relevance
Most high-risk trauma patients injured in rural areas were cared for outside of major trauma centers and most rural trauma deaths occurred early, although overall mortality did not differ between regions. There are opportunities for improved timeliness and access to major trauma care among patients injured in rural regions.
-
Subjects:
-
Source:JAMA Surg. 152(1):11-18.
-
Pubmed ID:27732713
-
Pubmed Central ID:PMC5409522
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:152
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha256:1be6f672b685328d940bc1c705e07d4d01c4fe190d07da33bc921a6b4788a981
-
Download URL:
-
File Type:
 [PDF
- 470.55 KB
]
[PDF
- 470.55 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access