Refractory Status Epilepticus in Children: intention-to-treat with continuous infusions of midazolam and pentobarbital
Supporting Files

-
Oct 2016
-
File Language:
English
Details
-
Alternative Title:Pediatr Crit Care Med
-
Personal Author:Tasker, Robert C ; Goodkin, Howard P ; Fernández, Iván Sánchez ; Chapman, Kevin E ; Abend, Nicholas S ; Arya, Ravindra ; Brenton, James N ; Carpenter, Jessica L ; Gaillard, William D ; Glauser, Tracy A ; Goldstein, Joshua ; Helseth, Ashley R ; Jackson, Michele C ; Kapur, Kush ; Mikati, Mohamad A ; Peariso, Katrina ; Wainwright, Mark S ; Wilfong, Angus A ; Williams, Korwyn ; Loddenkemper, Tobias
-
Description:Objective
To describe pediatric patients with convulsive refractory status epilepticus (RSE) in whom there is intention-to-use an intravenous anesthetic for seizure control.
Design
Two-year prospective observational study evaluating patients (age range one month to 21 years) with RSE not responding to two antiepileptic drug classes and treated with continuous infusion of anesthetic agent.
Setting
Nine pediatric hospitals in the United States.
Patients
In a cohort of 111 patients with RSE (median age 3.7 years, 50% male), 54 (49%) underwent continuous infusion of anesthetic treatment.
Main Results
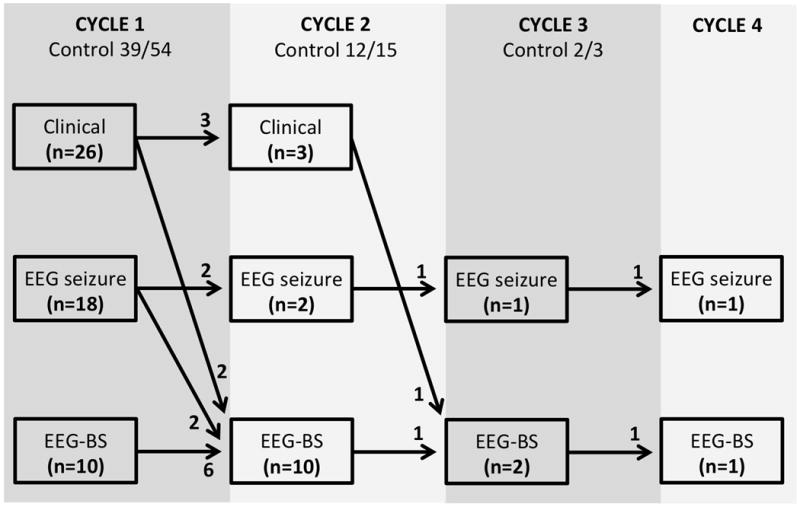
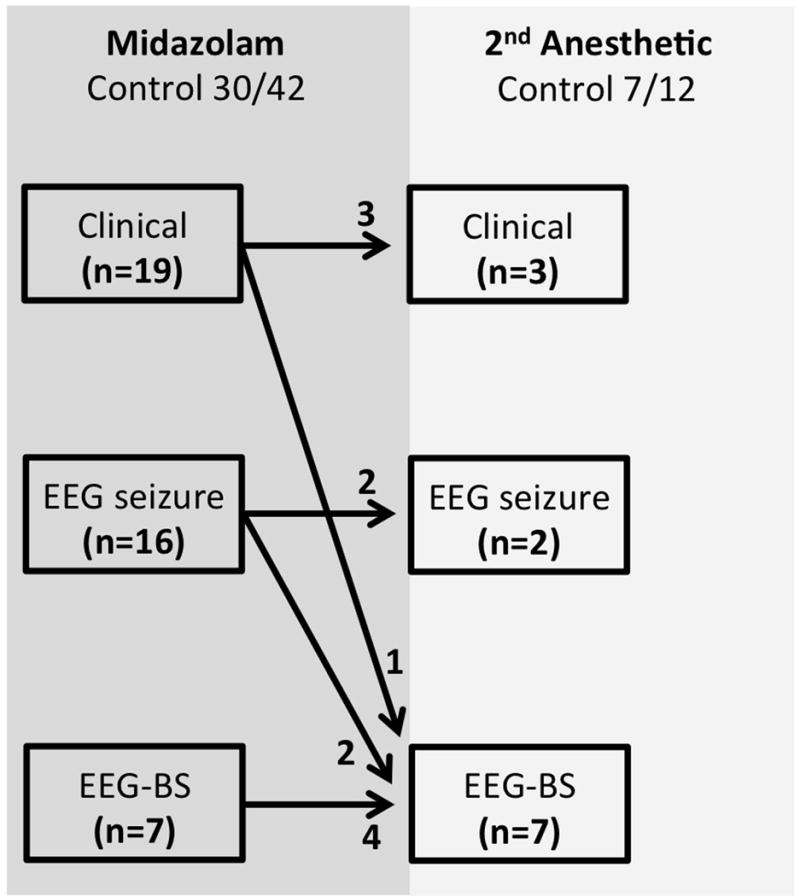
The median (interquartile range, IQR) intensive care unit length-of-stay was 10 (3–20) days. Up to four ‘cycles’ of serial anesthetic therapy were used and seizure termination was achieved in 94% by the second cycle. Seizure duration in controlled patients was 5.9 (1.9–34) hours for the first cycle, and longer when a second cycle was required (30 [4,−120] hours, p=0.048). Midazolam was the most frequent first-line anesthetic agent (78%); pentobarbital was the most frequently used second-line agent after midazolam failure (82%). An electroencephalographic endpoint was used in over half of the patients; higher midazolam dosing was used with a burst suppression endpoint. In midazolam non-responders, transition to a second agent occurred after a median of one day. Most patients (94%) experienced seizure termination with these two therapies.
Conclusions
Midazolam and pentobarbital remains the mainstay of continuous infusion therapy for RSE in the pediatric patient. The majority of patients experience seizure termination within a median of 30 hours. These data have implications for the design and feasibility of future intervention trials. That is, testing a new anesthetic anticonvulsant after failure of both midazolam and pentobarbital is unlikely to be feasible in a pediatric study, whereas a decision to test an alternative to pentobarbital, after midazolam failure, may be possible in a multicenter multinational study.
-
Subjects:
-
Source:Pediatr Crit Care Med. 17(10):968-975.
-
Pubmed ID:27500721
-
Pubmed Central ID:PMC5052105
-
Document Type:
-
Funding:
-
Volume:17
-
Issue:10
-
Collection(s):
-
Main Document Checksum:urn:sha256:e7ae081bf5b23c830baa1e3b005f1cdff6773d9d93c0978b80c10fe7213388d5
-
Download URL:
-
File Type:
 [PDF
- 248.72 KB
]
[PDF
- 248.72 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access