Optimizing Stroke Prevention in Patients With Atrial Fibrillation: A Cluster-Randomized Controlled Trial of a Computerized Antithrombotic Risk Assessment Tool in Australian General Practice, 2012–2013
Supporting Files
Public Domain

-
Jul 14 2016
-
File Language:
English
Details
-
Journal Article:Preventing Chronic Disease (PCD)
-
Personal Author:
-
Description:Introduction
Clinicians have expressed a need for tools to assist in selecting treatments for stroke prevention in patients with atrial fibrillation. The objective of this study was to evaluate the impact of a computerized antithrombotic risk assessment tool (CARAT) on general practitioners’ prescribing of antithrombotics for patients with atrial fibrillation.
Methods
A prospective, cluster-randomized controlled trial was conducted in 4 regions (in rural and urban settings) of general practice in New South Wales, Australia (January 2012–June 2013). General practitioner practices were assigned to an intervention arm (CARAT) or control arm (usual care). Antithrombotic therapy prescribing was assessed before and after application of CARAT.
Results
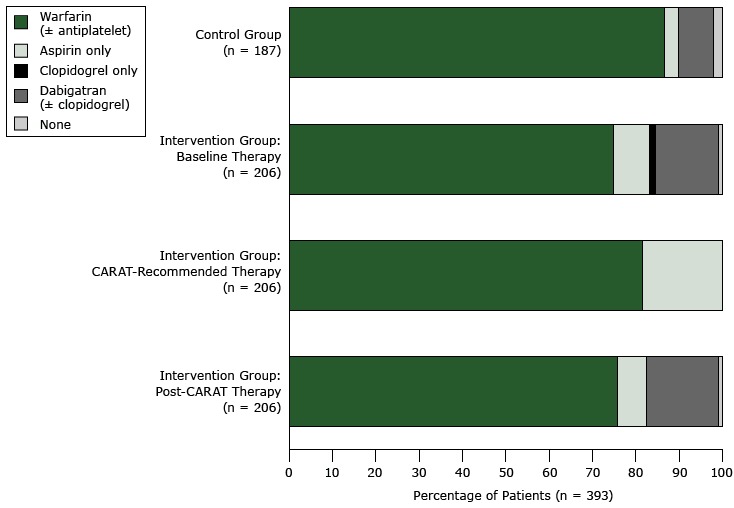
Overall, the antithrombotic therapies for 393 patients were reviewed by 48 general practitioners; we found no significant baseline differences in use of antithrombotics between the control arm and intervention arm. Compared with control patients, intervention patients (n = 206) were 3.1 times more likely to be recommended warfarin therapy (over any other treatment option; P < .001) and 2.8 times more likely to be recommended any anticoagulant (in preference to antiplatelet; P = .02). General practitioners agreed with most (75.2%) CARAT recommendations; CARAT recommended that 75 (36.4%) patients change therapy. After application of CARAT, the proportion of patients receiving any antithrombotic therapy was unchanged from baseline (99.0%); however, anticoagulant use increased slightly (from 89.3% to 92.2%), and antiplatelet use decreased (from 9.7% to 6.8%).
Conclusion
Tools such as CARAT can assist clinicians in selecting antithrombotic therapies, particularly in upgrading patients from antiplatelets to anticoagulants. However, the introduction of novel oral anticoagulants has complicated the decision-making process, and tools must evolve to weigh the risks and benefits of these new therapy options.
-
Subjects:
-
Source:Prev Chronic Dis. 13.
-
DOI:
-
ISSN:1545-1151
-
Pubmed ID:27418212
-
Pubmed Central ID:PMC4951074
-
Document Type:
-
Place as Subject:
-
Volume:13
-
Collection(s):
-
Main Document Checksum:urn:sha-512:ae83a98ee942102fe21a6527affdebc1e7f3c781504376fea4c3639d7d1e5944509173eaf039e3c3f6c0705a5e6d3e3d2c99cf3b54024c195806f2a145ae9103
-
Download URL:
-
File Type:
 [PDF
- 413.49 KB
]
[PDF
- 413.49 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Preventing Chronic Disease