Cost-effectiveness analysis of hepatocellular carcinoma screening by combinations of ultrasound and alpha-fetoprotein among Alaska Native people, 1983–2012
Supporting Files
Public Domain

-
May 18 2016
-
File Language:
English
Details
-
Alternative Title:Int J Circumpolar Health
-
Personal Author:
-
Description:Background
The American Association for the Study of Liver Diseases (AASLD) recommends semi-annual hepatocellular carcinoma (HCC) screening using ultrasound (U.S.) in persons with chronic hepatitis B (CHB) virus infection at high risk for HCC such as Asian males aged ≥40 years and Asian females aged ≥50 years
Objective
To analyze the cost-effectiveness of 2 HCC screening methods in the Alaska Native (AN) health system: US-alone, or screening by alpha-fetoprotein (AFP) initially and switching to US for subsequent screenings if AFP >10 ng/mL (AFP→US)
Design
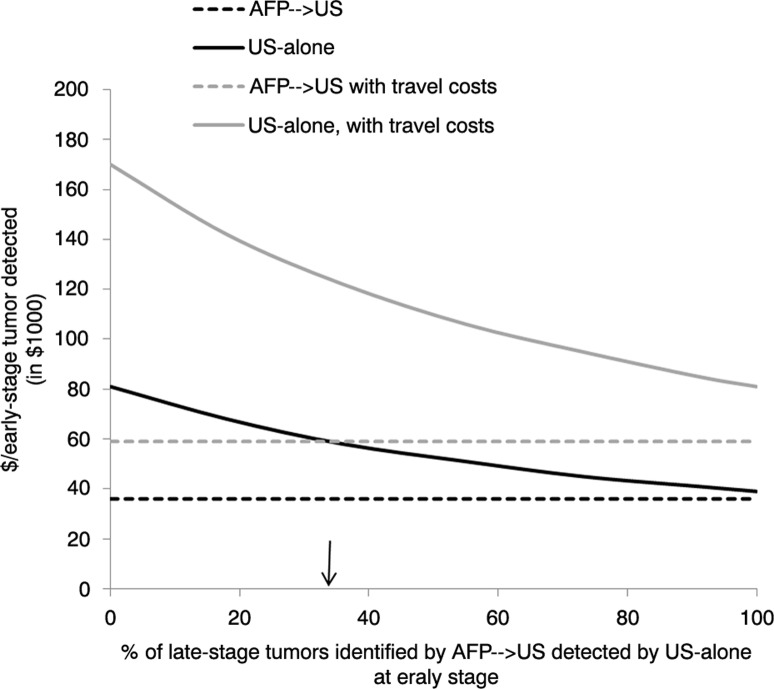
A spreadsheet-based model was developed for accounting the costs of 2 hypothetical HCC screening methods We used epidemiologic data from a cohort of 839 AN persons with CHB who were offered HCC screening by AFP/US semi-annually during 1983–2012 We assumed that compared with AFP→US, US-alone identifies 33% more tumors at an early stage (defined as a single tumor ≤5 cm or ≤3 tumors ≤3 cm in diameter) Years of life gained (YLG) attributed to screening was estimated by comparing additional years of survival among persons with early- compared with late-stage tumors Screening costs were calculated using Medicare reimbursement rates in 2012 Future screening costs and YLG were projected over a 30-year time horizon using a 3% discount rate
Results
The total cost of screening for the cohort by AFP→US would have been approximately $357,000 ($36,000/early-stage tumor detected) compared to $814,000 ($59,000/early-stage tumor detected) by US-alone The AFP→US method would have yielded an additional 278 YLG ($13,000/YLG) compared with 389 YLG ($21,000/YLG) for US-alone Screening by US-alone would incur an additional $114,000 per extra early-tumor detected compared with AFP→US and $41,000 per extra YLG
Conclusions
Although US-alone HCC screening might have yielded more YLG than AFP→US, the reduced costs of the AFP→US method could expand access to HCC screening in resource constrained settings
-
Subjects:
-
Source:Int J Circumpolar Health 2016; 75
-
Pubmed ID:27197711
-
Pubmed Central ID:PMC4873562
-
Document Type:
-
Volume:75
-
Collection(s):
-
Main Document Checksum:urn:sha256:01940ff6927cb89d877e7040a79725aa151f181421b0c3e3bbec3b6b079d643f
-
Download URL:
-
File Type:
 [PDF
- 356.71 KB
]
[PDF
- 356.71 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access