Retention in an antiretroviral therapy programme during an era of decreasing drug cost in Limbe, Cameroon
Supporting Files
Public Domain

-
Jun 16 2011
-
Details
-
Alternative Title:J Int AIDS Soc
-
Personal Author:
-
Description:Background
In 2002, Cameroon initiated scale up of antiretroviral therapy (ART); on 1 October 2004, a substantial reduction in ART cost occurred. We assessed the impact of this event and other factors on enrolment and retention in care among HIV-infected patients initiating ART from February 2002 to December 2005 at the single ART clinic serving the Southwest Region in Limbe, Cameroon.
Methods
We retrospectively analyzed clinical and pharmacy payment records of HIV-infected patients initiating ART according to national guidelines. We compared two cohorts of patients, enrolled before and after 1 October 2004, to determine if price reduction was associated with enhanced enrolment. We assessed factors associated with retention and survival by Cox proportional hazards models. Retention in care implied patients who had contact with the healthcare system as of 31 December 2005 (including those who were transferred to continue care in other ART centres), although these patients may have interrupted therapy at some time. A patient who was not retained in care may have dropped out (lost to follow up) or died.
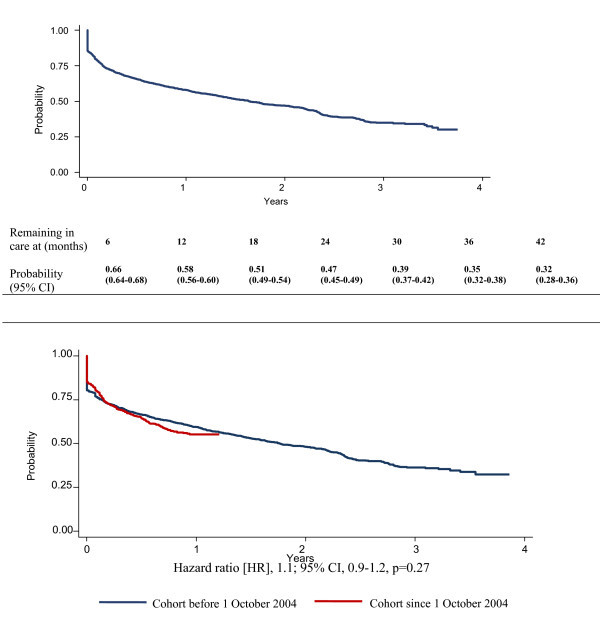
Results
Mean enrolment rates for 2920 patients who initiated ART before and after the price reduction were 46.5 and 95.5 persons/month, respectively (p < 0.001). The probabilities of remaining alive and in care were 0.66 (95% CI 0.64-0.68) at six months, 0.58 (95% CI 0.56-0.60) at one year, 0.47 (95% CI 0.45-0.49) at two years and 0.35 (95% CI 0.32-0.38) at three years; they were not significantly different between the two cohorts of patients enrolled before and after the price reduction over the first 15 months of comparable follow up (hazard ratio 1.1; 95% CI 0.9-1.2, p = 0.27). In multivariable analysis using multiple imputations to compensate for missing values, factors associated with dropping out of care or dying were male gender (HR 1.33 [1.18-1.50], p = 0.003), treatment paid by self, family or partly by other (HR 3.05 [1.99-4.67], p < 0.001), and, compared with residents of Limbe, living more than 150 km from Limbe (HR 1.41 [1.18-1.69], p < 0.001), or being residents of Douala (HR 1.51 [1.16-1.98], p < 0.001).
Conclusions
Reducing the cost of ART increased enrolment of clients in the programme, but did not change retention in care. In a system where most clients pay for ART, an accessible clinic location may be more important than the cost of medication for retention in care. Decentralizing ART clinics might improve retention and survival among patients on ART.
-
Subjects:
-
Source:J Int AIDS Soc. 2011; 14:32.
-
Pubmed ID:21679416
-
Pubmed Central ID:PMC3143073
-
Document Type:
-
Place as Subject:
-
Volume:14
-
Collection(s):
-
Main Document Checksum:urn:sha-512:a9d8a3250972bfcc46f8b9e0d94b2e94996be5d750c30c7732da6b30a0fdf50d1f9bbf3678b718c1ed01f0da76caebb6cecc3199da528453a6afda2b6732df53
-
Download URL:
-
File Type:
 [PDF
- 342.94 KB
]
[PDF
- 342.94 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access