Old and new cluster designs in emergency field surveys: in search of a one-fits-all solution
Supporting Files
Public Domain

-
Jul 08 2008
Details
-
Alternative Title:Emerg Themes Epidemiol
-
Personal Author:
-
Description:Introduction
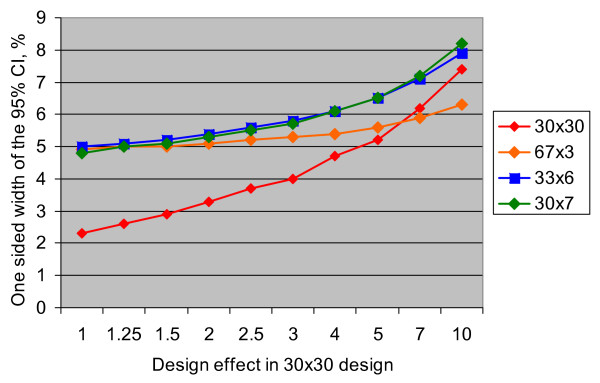
Cluster surveys are frequently used to measure key nutrition and health indicators in humanitarian emergencies. The survey design of 30 clusters of 7 children (30 × 7) was initially proposed by the World Health Organization for measuring vaccination coverage, and later a design of 30 clusters of 30 children (30 × 30) was introduced to measure acute malnutrition in emergency settings. Recently, designs of 33 clusters of 6 children (33 × 6) and 67 clusters of 3 children (67 × 3) have been proposed as alternatives that enable measurement of several key indicators with sufficient precision, while offering substantial savings in time. This paper explores expected effects of using 67 × 3, 33 × 6, or 30 × 7 designs instead of a "standard" 30 × 30 design on precision and accuracy of estimates, and on time required to complete the survey.
Analysis
The 67 × 3, 33 × 6, and 30 × 7 designs are expected to be more statistically efficient for measuring outcomes having high design effects (e.g., vaccination coverage, vitamin A distribution coverage, or access to safe water sources), and less efficient for measuring outcomes with more within-cluster variability, such as global acute malnutrition or anemia. Because of small sample sizes, these designs may not provide sufficient levels of precision to measure crude mortality rates. Given the small number (3 to 7) of survey subjects per cluster, it may be hard to select representative samples of subjects within clusters.
Conclusion
Cluster designs discussed in this paper may offer substantial time and cost savings compared to the traditional 30 × 30 design, and may provide acceptable levels of precision when measuring outcomes that have high intracluster homogeneity. Further investigation is required to determine whether these designs can consistently provide accurate point estimates for key outcomes of interest. Organizations conducting cluster surveys in emergency settings need to build their technical capacity in survey design to be able to calculate context-specific sample sizes individually for each planned survey.
-
Subjects:
-
Source:Emerg Themes Epidemiol. 2008; 5:7.
-
Document Type:
-
Volume:5
-
Collection(s):
-
Main Document Checksum:urn:sha256:4eede50cc1d159b39924e7dbe96997b15346a0637b34305c0a1bfe10ec0c12e4
-
Download URL:
-
File Type:
 [PDF
- 241.35 KB
]
[PDF
- 241.35 KB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access