Cost-effectiveness of a national population-based screening program for type 2 diabetes: the Brazil experience
Supporting Files
Public Domain

-
Oct 31 2015
-
Details
-
Alternative Title:Diabetol Metab Syndr
-
Personal Author:
-
Corporate Authors:
-
Description:Background
The cost-effectiveness of screening for type 2 diabetes mellitus (DM2) in developing countries remains unknown. The Brazilian government conducted a nationwide population screening program for type 2 diabetes mellitus (BNDSP) in which 22 million capillary glucose tests were performed in individuals aged 40 years and older. The objective of this study was to evaluate the life-time cost-effectiveness of a national population-based screening program for DM2 conducted in Brazil.
Methods
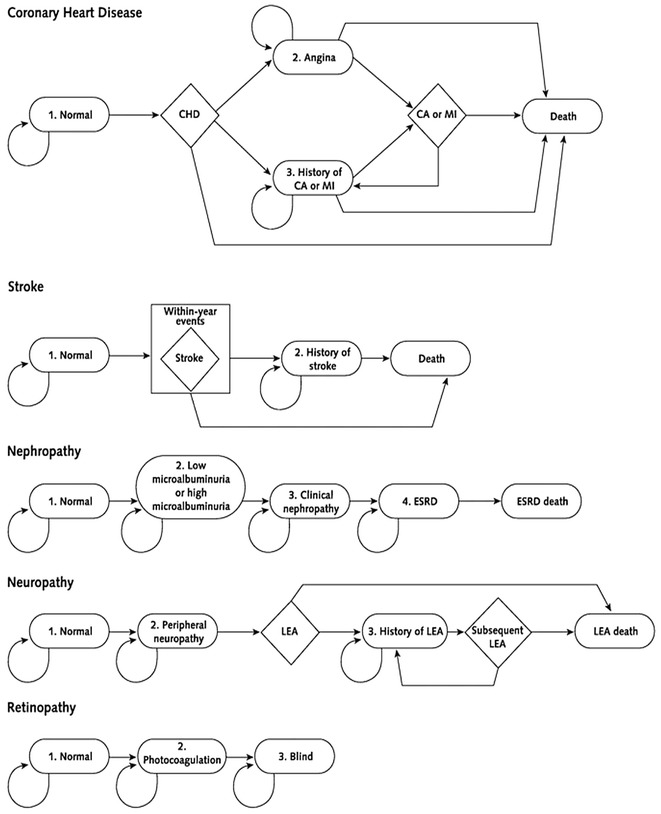
We used a Markov-based cost-effectiveness model to simulate the long-term costs and benefits of screening for DM2, compared to no screening program. The analysis was conducted from a public health care system perspective. Sensitivity analyses were conducted to examine the robustness of results to key model parameters.
Results
Brazilian National diabetes screening program will yield a large health benefit and higher costs. Compared with no screening, screen detection of undiagnosed diabetes resulted in US$ 31,147 per QALY gained. Results from sensitivity analyses found that screening targeted at hypertensive individuals would cost US$ 22,695/QALY. When benefits from early glycemic control on cardiovascular outcomes were considered, the cost per QALY gained would reduce significantly.
Conclusions
In the base case analysis, not considering the intangible benefit of transferring diabetes management to primary care nor the benefit of using statin to treat eligible diabetic patients, CE ratios were not cost-effective considering thresholds proposed by the World Health Organization. However, significant uncertainty was demonstrated in sensitivity analysis. Our results indicate that policy-makers should carefully balance the benefit and cost of the program while considering using a population-based approach to screen for diabetes.
-
Subjects:
-
Source:Diabetol Metab Syndr. 7.
-
Pubmed ID:26523154
-
Pubmed Central ID:PMC4628345
-
Document Type:
-
Volume:7
-
Collection(s):
-
Main Document Checksum:urn:sha256:a85437cbcab91160424d183baddc3e27c7a18a4688ebbd74b774bc06c751d688
-
Download URL:
-
File Type:
 [PDF
- 1.10 MB
]
[PDF
- 1.10 MB
]
Supporting Files

ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access