West Nile Virus: Review of the Literature
Supporting Files

-
7 17 2013
File Language:
English
Details
-
Alternative Title:JAMA
-
Personal Author:
-
Description:IMPORTANCE
Since its introduction in North America in 1999,West Nile virus has produced the 3 largest arboviral neuroinvasive disease outbreaks ever recorded in the United States.
OBJECTIVE
To review the ecology, virology, epidemiology, clinical characteristics, diagnosis, prevention, and control of West Nile virus, with an emphasis on North America.
EVIDENCE REVIEW
PubMed electronic database was searched through February 5, 2013. United States national surveillance data were gathered from the Centers for Disease Control and Prevention.
FINDINGS
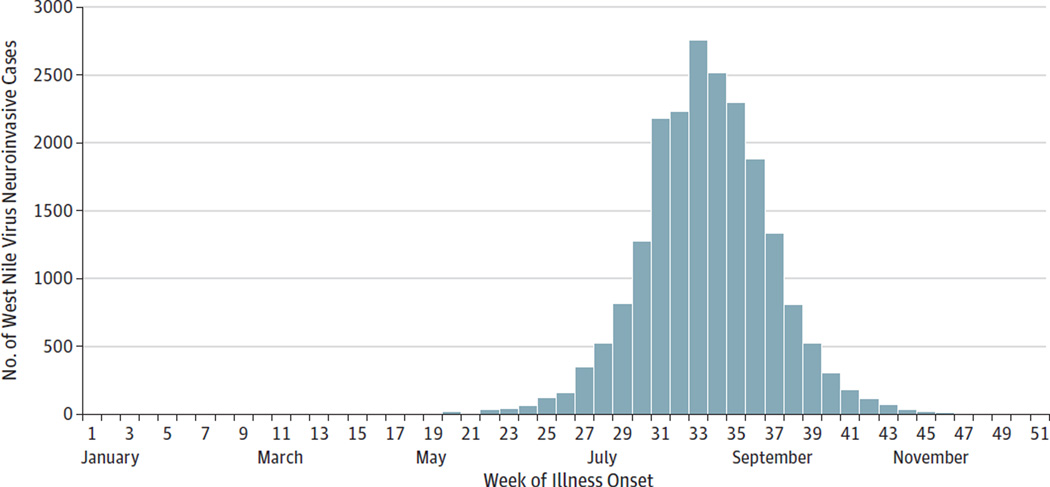
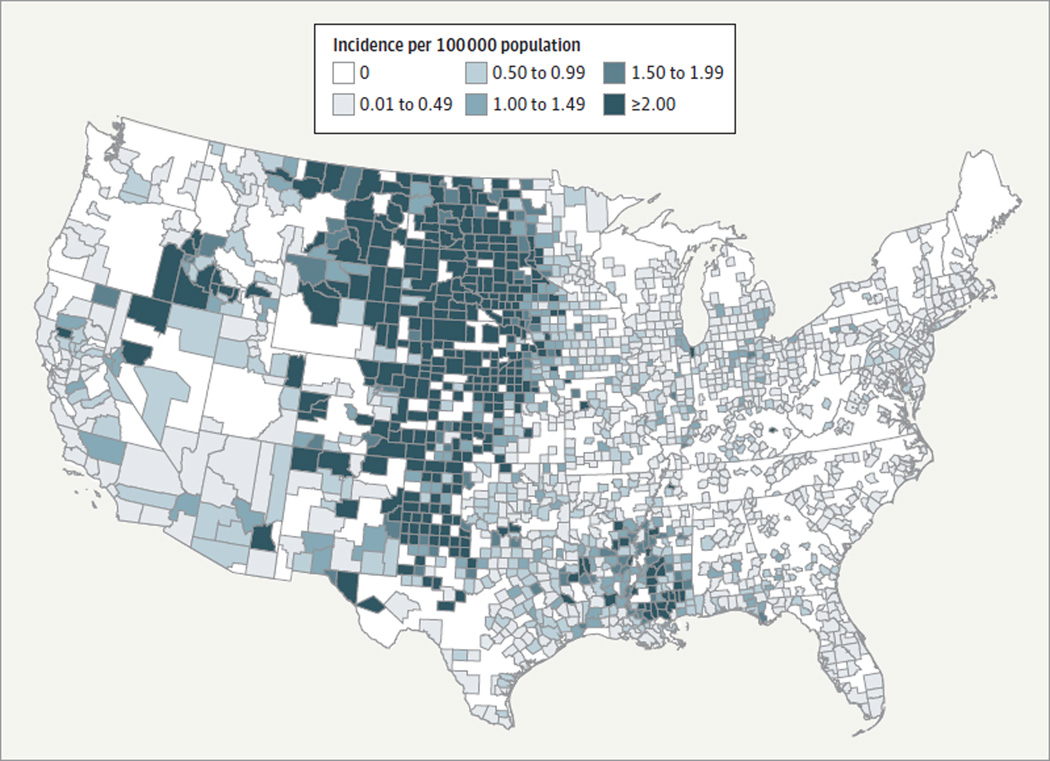
West Nile virus is now endemic throughout the contiguous United States, with 16 196 human neuroinvasive disease cases and 1549 deaths reported since 1999. More than 780 000 illnesses have likely occurred. To date, incidence is highest in the Midwest from mid-July to early September. West Nile fever develops in approximately 25% of those infected, varies greatly in clinical severity, and symptoms may be prolonged. Neuroinvasive disease (meningitis, encephalitis, acute flaccid paralysis) develops in less than 1% but carries a fatality rate of approximately 10%. Encephalitis has a highly variable clinical course but often is associated with considerable long-term morbidity. Approximately two-thirds of those with paralysis remain with significant weakness in affected limbs. Diagnosis usually rests on detection of IgM antibody in serum or cerebrospinal fluid. Treatment is supportive; no licensed human vaccine exists. Prevention uses an integrated pest management approach, which focuses on surveillance, elimination of mosquito breeding sites, and larval and adult mosquito management using pesticides to keep mosquito populations low. During outbreaks or impending outbreaks, emphasis shifts to aggressive adult mosquito control to reduce the abundance of infected, biting mosquitoes. Pesticide exposure and adverse human health events following adult mosquito control operations for West Nile virus appear negligible.
CONCLUSIONS AND RELEVANCE
In North America, West Nile virus has and will remain a formidable clinical and public health problem for years to come.
-
Subjects:
-
Source:JAMA. 310(3):308-315
-
Pubmed ID:23860989
-
Pubmed Central ID:PMC4563989
-
Document Type:
-
Funding:
-
Volume:310
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:17cd1b39bdba6a09b70840ee494e8e4f9bc9cf8b579a13a51b2ebb11b04404f8
-
Download URL:
-
File Type:
 [PDF
- 1.23 MB
]
[PDF
- 1.23 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access