Myocardial edema as detected by pre-contrast T1 and T2 MRI delineates area at risk associated with acute myocardial infarction
Supporting Files

-
6-2012
-
File Language:
English
Details
-
Alternative Title:JACC Cardiovasc Imaging
-
Personal Author:
-
Description:Objectives
To determine whether cardiac magnetic resonance (CMR) in vivo T1-mapping can measure myocardial area at risk (AAR) compared with microspheres or T2-mapping CMR.
Background
If T2-weighted CMR is abnormal in the AAR due to edema related to myocardial ischemia, then T1-weighted CMR should also be able to detect and accurately quantify AAR.
Methods
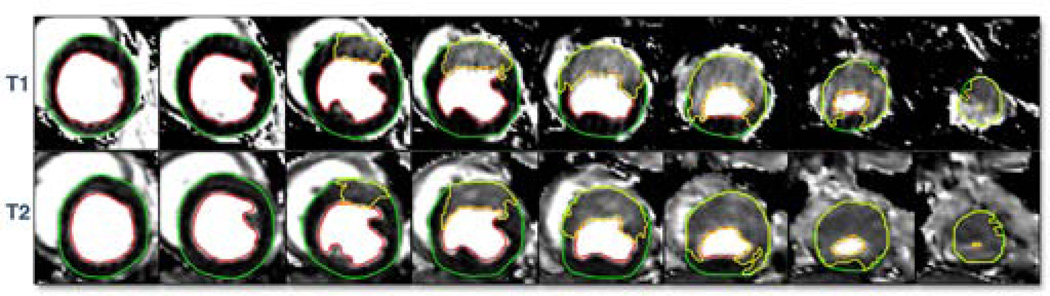
Dogs (n=9) underwent a 2 hour coronary occlusion followed by 4 hours of reperfusion. CMR of the left ventricle was performed for mapping of T1 and T2 prior to any contrast administration. AAR was defined as regions which had a T1 or T2 value (ms) greater than 2SD from remote, and regions with microsphere blood flow (ml/min/g) during occlusion less than 2SD from remote. Infarct size was determined by triphenyltetrazolium chloride staining.
Results
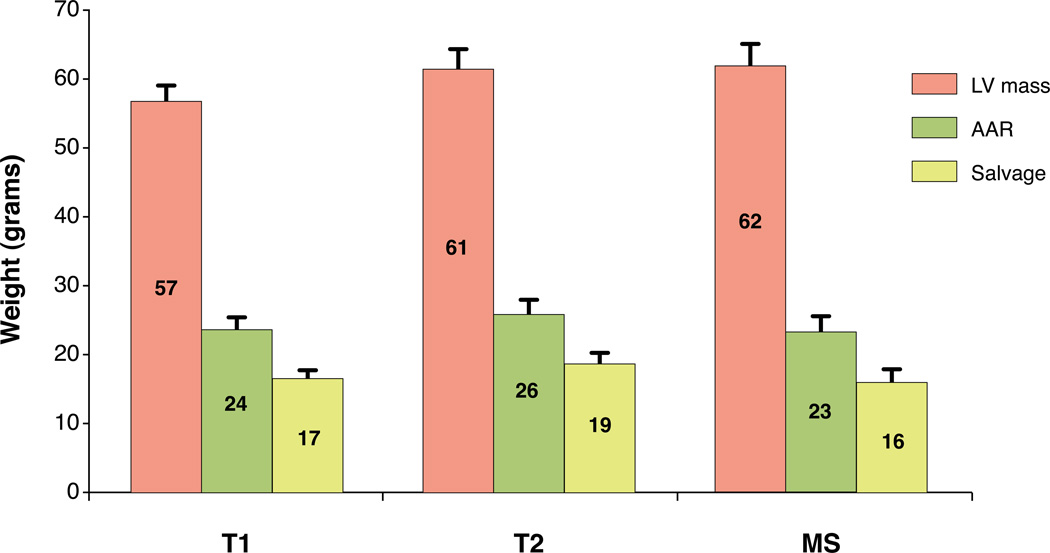
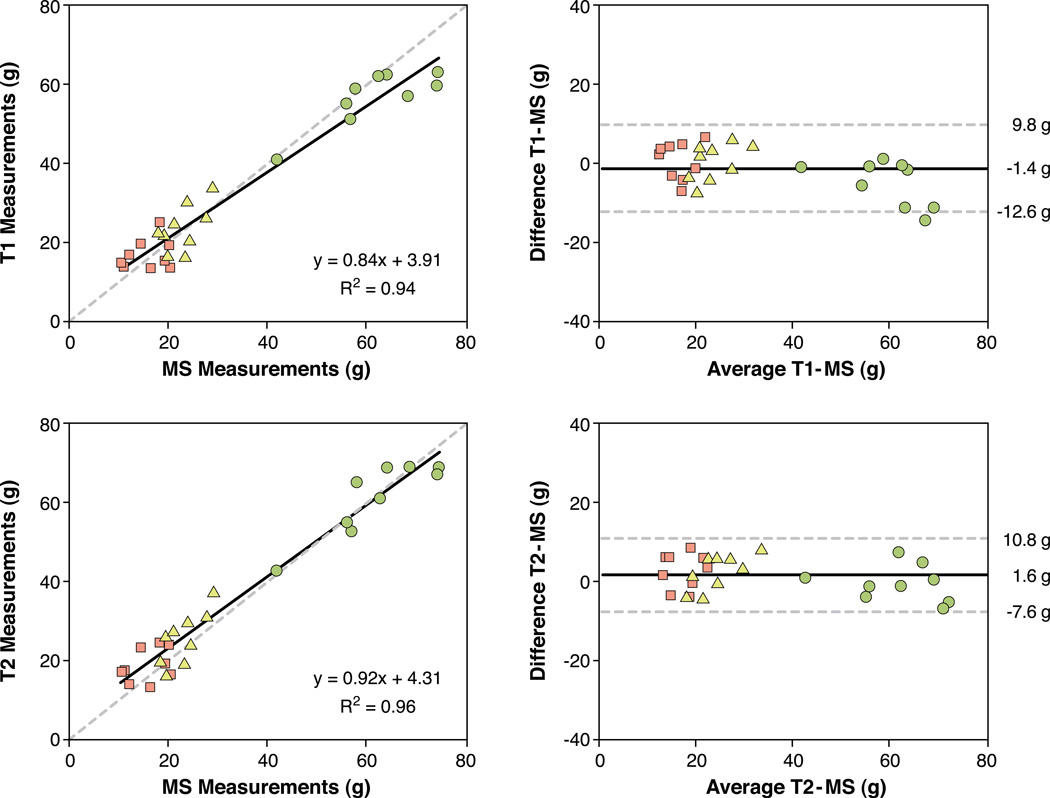
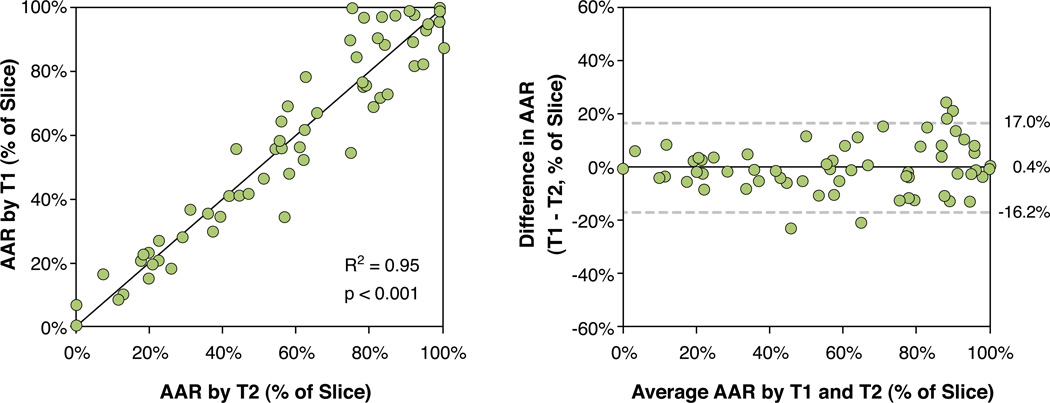
The relaxation parameters T1 and T2 were increased in the AAR compared to remote myocardium (T1: 1133±55 vs. 915±33ms, T2: 71±6 vs. 49±3 ms; mean±SD). On a slice-by-slice basis (n=78 slices), AAR by T1- and T2-mapping correlated (R2=0.95, p<0.001) with good agreement (0.4±16.6 % of slice, mean±2SD). On a whole-heart analysis, T1 measurements of left ventricular mass, AAR and myocardial salvage correlated to microsphere measures (R2=0.94) with good agreement (−1.4±11.2 g of myocardium; mean±2SD). Corresponding T2 measurements of left ventricular mass, AAR, and salvage correlated to microsphere analysis (R2=0.96, agreement 1.6±9.2 g of myocardium; mean±2SD). Median infarct size was 30% of the AAR (range 12–52).
Conclusions
For determining area at risk after acute myocardial infarction, non-contrast T1-mapping and T2-mapping sequences yield similar quantitative results, and both agree well with microspheres. The relaxation properties T1 and T2 both change in a way that is consistent with the presence of myocardial edema following myocardial ischemia/reperfusion.
-
Keywords:
-
Source:JACC Cardiovasc Imaging. 2012; 5(6):596-603
-
Pubmed ID:22698528
-
Pubmed Central ID:PMC3769169
-
Document Type:
-
Funding:ZIA HL004607/ImNIH/Intramural NIH HHSUnited States/ ; ZIA HL004607-14/ImNIH/Intramural NIH HHSUnited States/ ; ZIA HL006136-02/ImNIH/Intramural NIH HHSUnited States/ ; HL-CR-05-004/HL/NHLBI NIH HHSUnited States/ ; 1 Z01 HL004607-08 CE/CE/NCIPC CDC HHSUnited States/ ; Z01 HL004607/ImNIH/Intramural NIH HHSUnited States/ ; ZIA HL006136-01/ImNIH/Intramural NIH HHSUnited States/ ; ZIA HL006136/ImNIH/Intramural NIH HHSUnited States/
-
Volume:5
-
Issue:6
-
Collection(s):
-
Main Document Checksum:urn:sha256:110367fa04228d8e901bb7e8f9beae1f0ac7e5ba4a8e1d31e646db77462de5db
-
Download URL:
-
File Type:
 [PDF
- 1.61 MB
]
[PDF
- 1.61 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access