First population-level effectiveness evaluation of a national programme to prevent HIV transmission from mother to child, South Africa
Supporting Files
Public Domain

-
Nov 04 2014
-
File Language:
English
Details
-
Alternative Title:J Epidemiol Community Health
-
Personal Author:
-
Description:Background
There is a paucity of data on the national population-level effectiveness of preventing mother-to-child transmission (PMTCT) programmes in high-HIV-prevalence, resource-limited settings. We assessed national PMTCT impact in South Africa (SA), 2010.
Methods
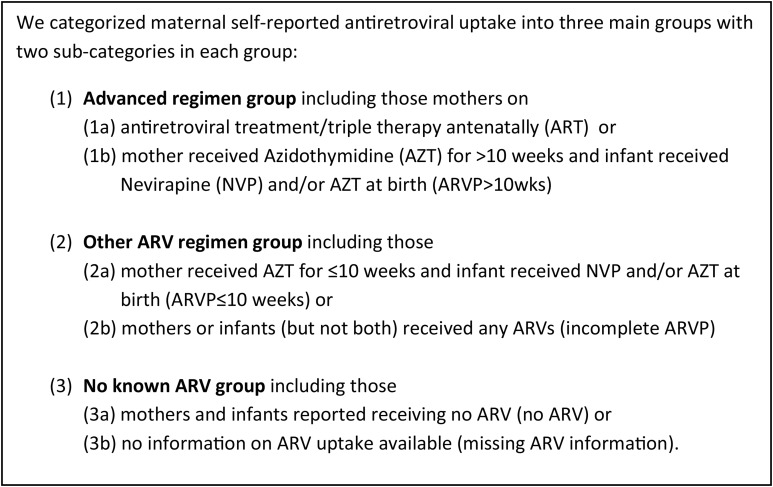
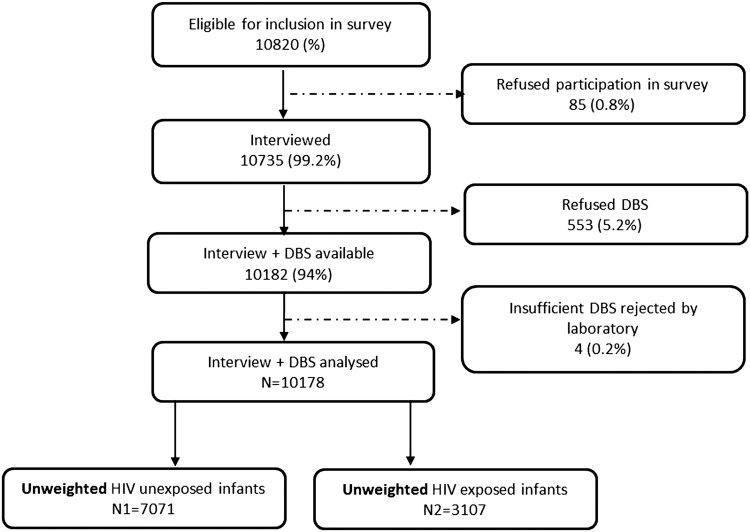
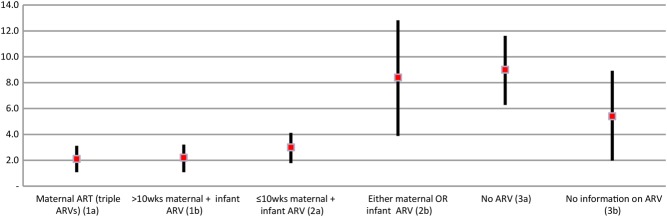
A facility-based survey was conducted using a stratified multistage, cluster sampling design. A nationally representative sample of 10 178 infants aged 4–8 weeks was recruited from 565 clinics. Data collection included caregiver interviews, record reviews and infant dried blood spots to identify HIV-exposed infants (HEI) and HIV-infected infants. During analysis, self-reported antiretroviral (ARV) use was categorised: 1a: triple ARV treatment; 1b: azidothymidine >10 weeks; 2a: azidothymidine ≤10 weeks; 2b: incomplete ARV prophylaxis; 3a: no antenatal ARV and 3b: missing ARV information. Findings were adjusted for non-response, survey design and weighted for live-birth distributions.
Results
Nationally, 32% of live infants were HEI; early mother-to-child transmission (MTCT) was 3.5% (95% CI 2.9% to 4.1%). In total 29.4% HEI were born to mothers on triple ARV treatment (category 1a) 55.6% on prophylaxis (1b, 2a, 2b), 9.5% received no antenatal ARV (3a) and 5.5% had missing ARV information (3b). Controlling for other factors groups, 1b and 2a had similar MTCT to 1a (Ref; adjusted OR (AOR) for 1b, 0.98, 0.52 to 1.83; and 2a, 1.31, 0.69 to 2.48). MTCT was higher in group 2b (AOR 3.68, 1.69 to 7.97). Within group 3a, early MTCT was highest among breastfeeding mothers 11.50% (4.67% to 18.33%) for exclusive breast feeding, 11.90% (7.45% to 16.35%) for mixed breast feeding, and 3.45% (0.53% to 6.35%) for no breast feeding). Antiretroviral therapy or >10 weeks prophylaxis negated this difference (MTCT 3.94%, 1.98% to 5.90%; 2.07%, 0.55% to 3.60% and 2.11%, 1.28% to 2.95%, respectively).
Conclusions
SA, a high-HIV-prevalence middle income country achieved <5% MTCT by 4–8 weeks post partum. The long-term impact on PMTCT on HIV-free survival needs urgent assessment.
-
Subjects:
-
Source:J Epidemiol Community Health. 2015; 69(3):240-248.
-
Document Type:
-
Place as Subject:
-
Volume:69
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:a457823d6fe1ad0c8421f9d701e97e4c574f8425df0df2695b0fcfcc48629424
-
Download URL:
-
File Type:
 [PDF
- 1.12 MB
]
[PDF
- 1.12 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access