Multicenter Evaluation of a Novel Surveillance Paradigm for Complications of Mechanical Ventilation
Supporting Files

-
Mar 22 2011
-
File Language:
English
Details
-
Alternative Title:PLoS One
-
Personal Author:
-
Corporate Authors:
-
Description:Background
Ventilator-associated pneumonia (VAP) surveillance is time consuming, subjective, inaccurate, and inconsistently predicts outcomes. Shifting surveillance from pneumonia in particular to complications in general might circumvent the VAP definition's subjectivity and inaccuracy, facilitate electronic assessment, make interfacility comparisons more meaningful, and encourage broader prevention strategies. We therefore evaluated a novel surveillance paradigm for ventilator-associated complications (VAC) defined by sustained increases in patients' ventilator settings after a period of stable or decreasing support.
Methods
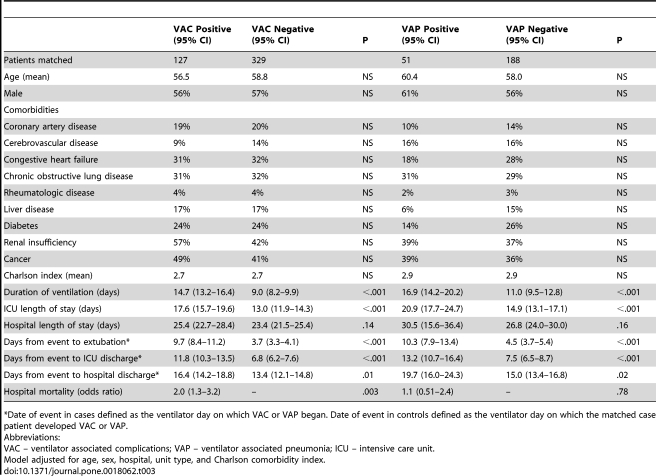
We assessed 600 mechanically ventilated medical and surgical patients from three hospitals. Each hospital contributed 100 randomly selected patients ventilated 2–7 days and 100 patients ventilated >7 days. All patients were independently assessed for VAP and for VAC. We compared incidence-density, duration of mechanical ventilation, intensive care and hospital lengths of stay, hospital mortality, and time required for surveillance for VAP and for VAC. A subset of patients with VAP and VAC were independently reviewed by a physician to determine possible etiology.
Results
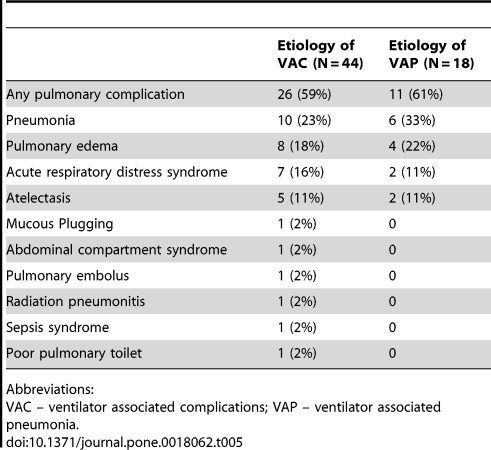
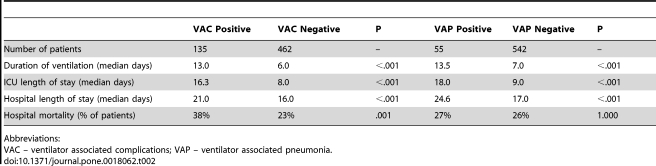
Of 597 evaluable patients, 9.3% had VAP (8.8 per 1,000 ventilator days) and 23% had VAC (21.2 per 1,000 ventilator days). Compared to matched controls, both VAP and VAC prolonged days to extubation (5.8, 95% CI 4.2–8.0 and 6.0, 95% CI 5.1–7.1 respectively), days to intensive care discharge (5.7, 95% CI 4.2–7.7 and 5.0, 95% CI 4.1–5.9), and days to hospital discharge (4.7, 95% CI 2.6–7.5 and 3.0, 95% CI 2.1–4.0). VAC was associated with increased mortality (OR 2.0, 95% CI 1.3–3.2) but VAP was not (OR 1.1, 95% CI 0.5–2.4). VAC assessment was faster (mean 1.8 versus 39 minutes per patient). Both VAP and VAC events were predominantly attributable to pneumonia, pulmonary edema, ARDS, and atelectasis.
Conclusions
Screening ventilator settings for VAC captures a similar set of complications to traditional VAP surveillance but is faster, more objective, and a superior predictor of outcomes.
-
Subjects:
-
Source:PLoS One. 6(3).
-
Pubmed ID:21445364
-
Pubmed Central ID:PMC3062570
-
Document Type:
-
Funding:
-
Volume:6
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:f07c1dd9982507a2c31f41bb8b28f46e733c6f07ad1b60e8270c6f28862cf77e
-
Download URL:
-
File Type:
 [PDF
- 181.71 KB
]
[PDF
- 181.71 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access