How to handle mortality when investigating length of hospital stay and time to clinical stability
Supporting Files

-
Oct 26 2011
-
File Language:
English
Details
-
Alternative Title:BMC Med Res Methodol
-
Personal Author:
-
Description:Background
Hospital length of stay (LOS) and time for a patient to reach clinical stability (TCS) have increasingly become important outcomes when investigating ways in which to combat Community Acquired Pneumonia (CAP). Difficulties arise when deciding how to handle in-hospital mortality. Ad-hoc approaches that are commonly used to handle time to event outcomes with mortality can give disparate results and provide conflicting conclusions based on the same data. To ensure compatibility among studies investigating these outcomes, this type of data should be handled in a consistent and appropriate fashion.
Methods
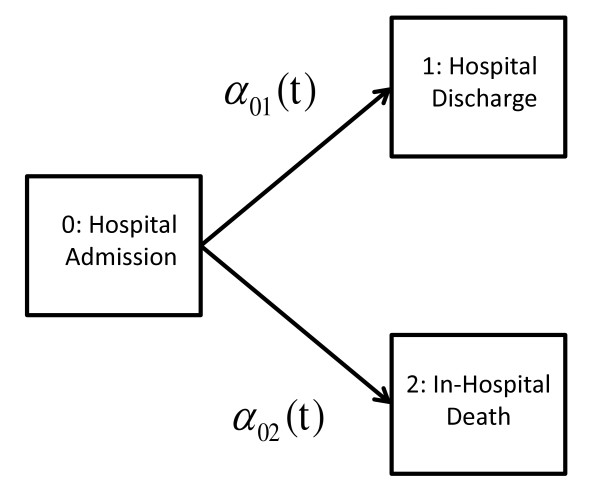
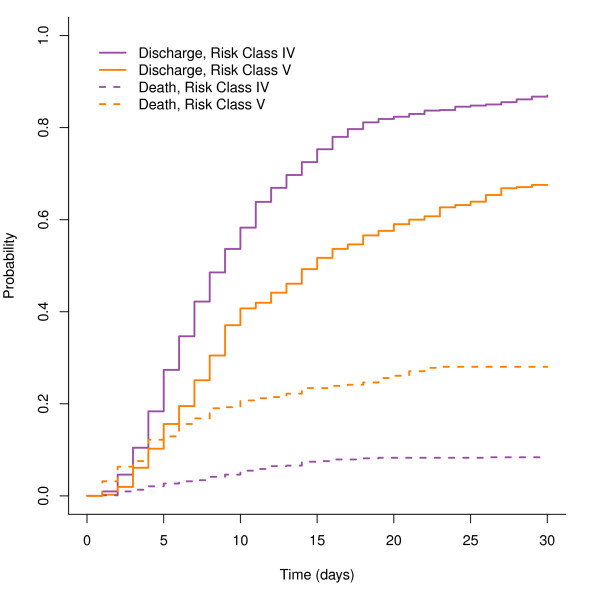
Using both simulated data and data from the international Community Acquired Pneumonia Organization (CAPO) database, we evaluate two ad-hoc approaches for handling mortality when estimating the probability of hospital discharge and clinical stability: 1) restricting analysis to those patients who lived, and 2) assigning individuals who die the "worst" outcome (right-censoring them at the longest recorded LOS or TCS). Estimated probability distributions based on these approaches are compared with right-censoring the individuals who died at time of death (the complement of the Kaplan-Meier (KM) estimator), and treating death as a competing risk (the cumulative incidence estimator). Tests for differences in probability distributions based on the four methods are also contrasted.
Results
The two ad-hoc approaches give different estimates of the probability of discharge and clinical stability. Analysis restricted to patients who survived is conceptually problematic, as estimation is conditioned on events that happen at a future time. Estimation based on assigning those patients who died the worst outcome (longest LOS and TCS) coincides with the complement of the KM estimator based on the subdistribution hazard, which has been previously shown to be equivalent to the cumulative incidence estimator. However, in either case the time to in-hospital mortality is ignored, preventing simultaneous assessment of patient mortality in addition to LOS and/or TCS. The power to detect differences in underlying hazards of discharge between patient populations differs for test statistics based on the four approaches, and depends on the underlying hazard ratio of mortality between the patient groups.
Conclusions
Treating death as a competing risk gives estimators which address the clinical questions of interest, and allows for simultaneous modelling of both in-hospital mortality and TCS / LOS. This article advocates treating mortality as a competing risk when investigating other time related outcomes.
-
Subjects:
-
Source:BMC Med Res Methodol. 2011; 11:144.
-
Pubmed ID:22029846
-
Pubmed Central ID:PMC3269825
-
Document Type:
-
Funding:
-
Volume:11
-
Collection(s):
-
Main Document Checksum:urn:sha256:5781de57677ce428a09c33cc8c8fb6404b41c40f043126b6e5ad505658dc4d6a
-
Download URL:
-
File Type:
 [PDF
- 479.62 KB
]
[PDF
- 479.62 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access