Secondary Prevention of Myocardial Infarction With Nonpharmacologic Strategies in a Medicaid Cohort
Supporting Files
Public Domain

-
Mar 16 2009
-
File Language:
English
Details
-
Journal Article:Preventing Chronic Disease (PCD)
-
Personal Author:
-
Description:Background
The quality of health care after myocardial infarction (MI) may be lacking; in particular, guidelines for nonpharmacologic interventions (cardiac rehabilitation, smoking cessation) may receive insufficient priority. We identified gaps between secondary prevention guidelines and ambulatory care received by Medicaid enrollees after an MI.
Methods
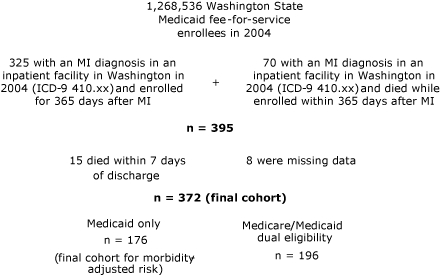
MI survivors were selected by using 2004 Washington State Medicaid administrative claims. Deidentified data were abstracted for hospitalizations, ambulatory care, and prescriptions for 365 days after the MI. Cox regression analysis compared utilization of guideline-directed secondary prevention strategies with death and recurrent hospitalization.
Results
The sample size was 372. Fifty patients died during the year after the MI, and 144 were rehospitalized. Only 2 patients attended a cardiac rehabilitation program. Tobacco cessation counseling was associated with a 66% reduction in death, but only 72.6% of smokers were counseled. Less than half (45.4%) of patients saw a primary care provider within 90 days of their MI, and 7.5% never contacted a health care provider. Receiving regular primary care was associated with a decreased risk for death (hazard ratio, 0.91; 95% confidence interval, 0.84-0.97, P < .01). A protective trend was associated with care by a cardiologist, but only 21.5% received specialist care.
Conclusion
Analysis of Medicaid claims data suggests rates of secondary prevention are less than optimal. To improve survival and reduce rehospitalization after an MI, policy changes (tobacco cessation benefits, expansion of rehabilitation programs), health care capacity (training, referral patterns, and coordination of care), and improvements to access (removing barriers, increasing facilities, targeting minority populations) could be implemented.
-
Subjects:
-
Source:Prev Chronic Dis. 2009; 6(2).
-
ISSN:1545-1151
-
Document Type:
-
Place as Subject:
-
Location:
-
Volume:6
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha-512:b379334ea130550e678ebcfbccaa13aeeee723cefd4a34d81ed9172791a51965ff901985eb3487601d7b60fe4d493ff4a8510d726897e3886dfb8a86f49fc26e
-
Download URL:
-
File Type:
 [PDF
- 459.98 KB
]
[PDF
- 459.98 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Preventing Chronic Disease