Implementation and outcomes of a clinician-directed intervention to improve antibiotic prescribing for acute respiratory tract infections within the Veterans’ Affairs Healthcare System
Supporting Files

-
5 2023
-
File Language:
English
Details
-
Alternative Title:Infect Control Hosp Epidemiol
-
Personal Author:
-
Description:Objective:
To determine whether a clinician-directed acute respiratory tract infection (ARI) intervention was associated with improved antibiotic prescribing and patient outcomes across a large US healthcare system.
Design:
Multicenter retrospective quasi-experimental analysis of outpatient visits with a diagnosis of uncomplicated ARI over a 7-year period.
Participants:
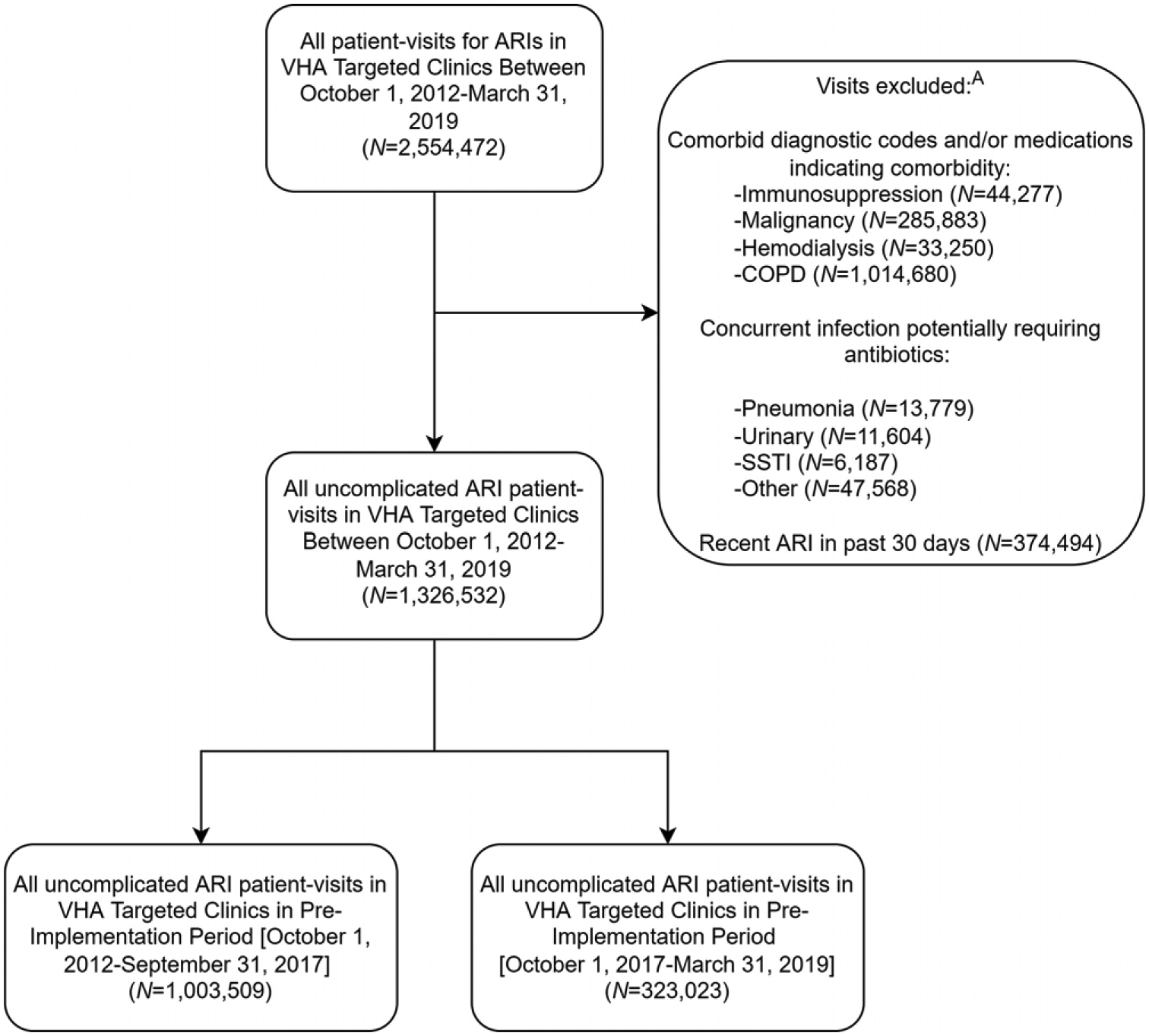
Outpatients with ARI diagnoses: sinusitis, pharyngitis, bronchitis, and unspecified upper respiratory tract infection (URI-NOS). Outpatients with concurrent infection or select comorbid conditions were excluded.
Intervention(s):
Audit and feedback with peer comparison of antibiotic prescribing rates and academic detailing of clinicians with frequent ARI visits. Antimicrobial stewards and academic detailing personnel delivered the intervention; facility and clinician participation were voluntary.
Measure(s):
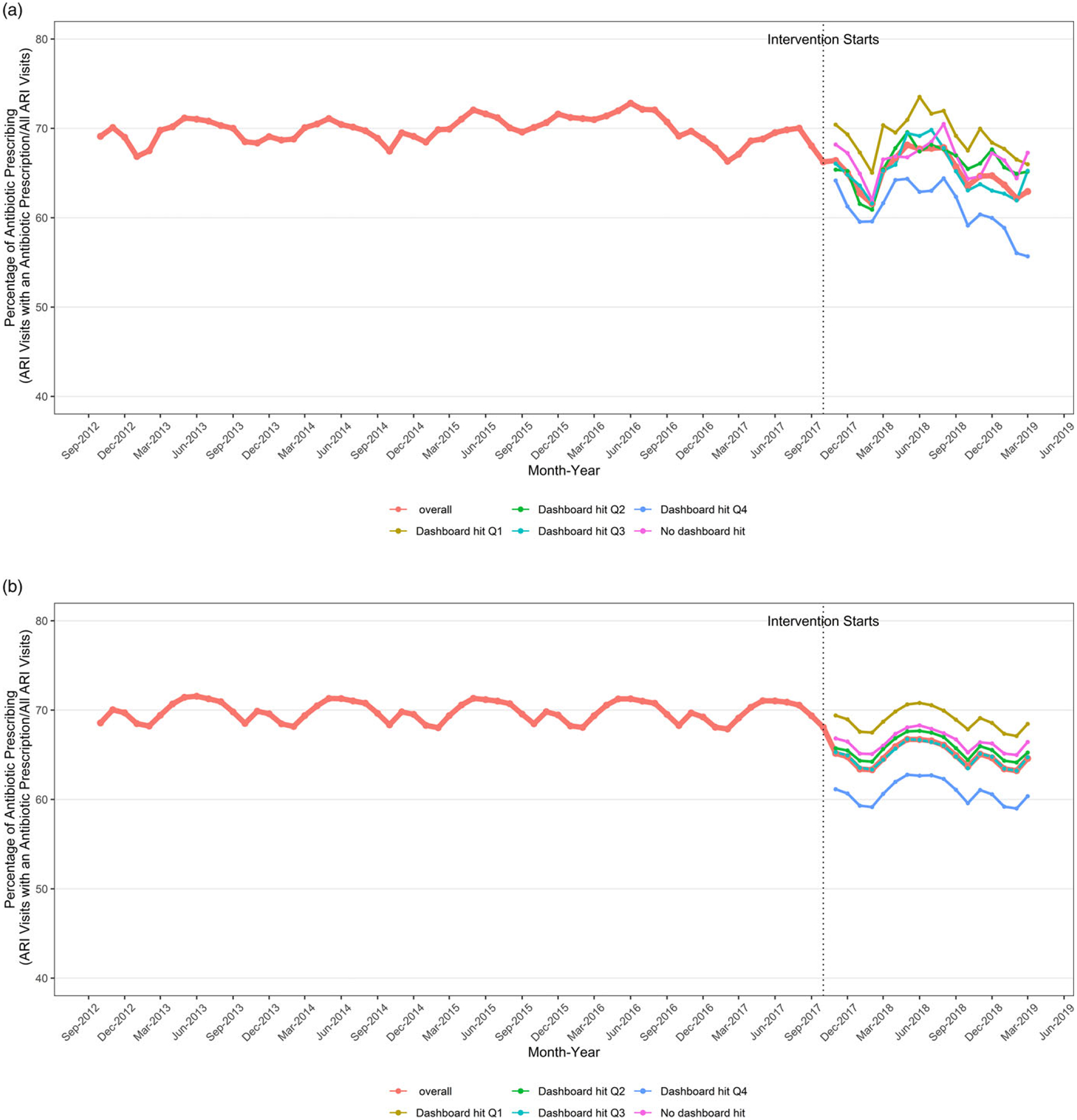
We calculated the probability to receive antibiotics for an ARI before and after implementation. Secondary outcomes included probability for a return clinic visits or infection-related hospitalization, before and after implementation. Intervention effects were assessed with logistic generalized estimating equation models. Facility participation was tracked, and results were stratified by quartile of facility intervention intensity.
Results:
We reviewed 1,003,509 and 323,023 uncomplicated ARI visits before and after the implementation of the intervention, respectively. The probability to receive antibiotics for ARI decreased after implementation (odds ratio [OR], 0.82; 95% confidence interval [CI], 0.78–0.86). Facilities with the highest quartile of intervention intensity demonstrated larger reductions in antibiotic prescribing (OR, 0.69; 95% CI, 0.59–0.80) compared to nonparticipating facilities (OR, 0.89; 95% CI, 0.73–1.09). Return visits (OR, 1.00; 95% CI, 0.94–1.07) and infection-related hospitalizations (OR, 1.21; 95% CI, 0.92–1.59) were not different before and after implementation within facilities that performed intensive implementation.
Conclusions:
Implementation of a nationwide ARI management intervention (ie, audit and feedback with academic detailing) was associated with improved ARI management in an intervention intensity–dependent manner. No impact on ARI-related clinical outcomes was observed.
-
Keywords:
-
Source:Infect Control Hosp Epidemiol. 44(5):746-754
-
Pubmed ID:35968847
-
Pubmed Central ID:PMC10882581
-
Document Type:
-
Funding:
-
Volume:44
-
Issue:5
-
Collection(s):
-
Main Document Checksum:urn:sha256:0c5f58762d631b47bc1f58e4c515367f31e246ea97337ad73fe97572a6c583ab
-
Download URL:
-
File Type:
 [PDF
- 566.39 KB
]
[PDF
- 566.39 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access