Achieving Reductions in Opioid Dispensing: A Qualitative Comparative Analysis of State-Level Efforts to Improve Prescribing
Supporting Files

-
2023
-
File Language:
English
Details
-
Alternative Title:J Public Health Manag Pract
-
Personal Author:
-
Description:Objective.
To determine whether any combination of state-level public health activities were necessary or sufficient to reduce prescription opioid dispensing.
Design.
We examined 2016–2019 annual progress reports, 2014–2019 national opioid dispensing data (IQVIA), and interview data from states to categorize activities. We used crisp-set Qualitative Comparative Analysis (QCA) to determine which program activities, individually or in combination, were necessary or sufficient for a better than average decrease in morphine milligram equivalent (MME) per capita.
Setting.
29 U.S. state health departments
Participants.
State health departments implementing CDC’s Prevention for States (PfS) program
Main outcome.
Combinations of prevention activities related to changes in the rate of prescription opioid MME per capita dispensing from 2014 to 2019.
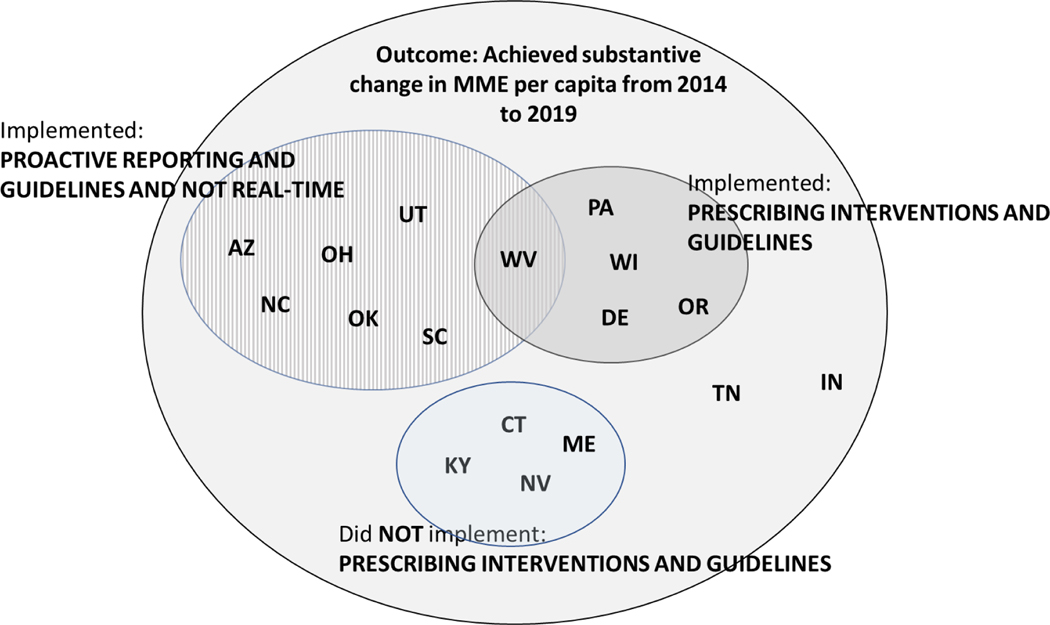
Results.
Three combinations were sufficient for greater than average state-level reductions in MME per capita: (1) Expanding and improving proactive reporting in combination with enhancing the uptake of evidence-based opioid prescribing guidelines and not moving toward a real-time PDMP; (2) Implementing or improving prescribing interventions for insurers, health systems, or pharmacy benefit managers in combination with enhancing the uptake of evidence-based opioid prescribing guidelines; (3) Not implementing or improving prescribing interventions for insurers, health systems, or pharmacy benefit managers in combination with not enhancing the uptake of evidence-based opioid prescribing guidelines. Interview data suggested that the three combinations indicate how state contexts and history with addressing opioid overdose shaped programming and the ability to reduce MME per capita.
Conclusions.
States successful in reducing opioid dispensing selected activities that built upon existing policies and interventions, which may indicate thoughtful use of resources. To maximize impact in addressing the opioid overdose epidemic, states and agencies may benefit from building on existing policies and interventions.
-
Keywords:
-
Source:J Public Health Manag Pract. 29(2):262-270
-
Pubmed ID:36112160
-
Pubmed Central ID:PMC9892169
-
Document Type:
-
Funding:
-
Volume:29
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha256:6e86208023788bc85f8bffe1dabc97ee81c7da1b0df331cabc9df1d7a88ddff1
-
Download URL:
-
File Type:
 [PDF
- 301.68 KB
]
[PDF
- 301.68 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access