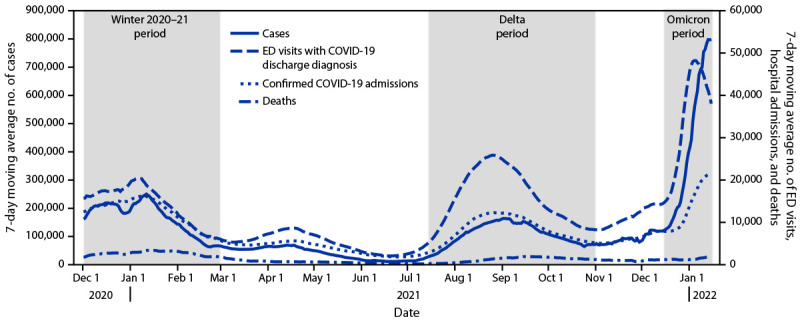
Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods — United States, December 2020–January 2022
Supporting Files
Public Domain

-
2022/01/28
-
File Language:
English
Details
-
Journal Article:Morbidity and Mortality Weekly Report
-
Personal Author:Iuliano, A. Danielle ; Brunkard, Joan M. ; Boehmer, Tegan K. ; Peterson, Elisha ; Adjei, Stacey ; Binder, Alison M. ; Cobb, Stacy ; Graff, Philip ; Hidalgo, Pauline ; Panaggio, Mark J. ; Rainey, Jeanette J. ; Rao, Preetika ; Soetebier, Karl ; Wacaster, Susan ; Ai, ChinEn ; Gupta, Vikas ; Molinari, Noelle-Angelique M. ; Ritchey, Matthew D.
-
Description:What is already known about this topic? The SARS-CoV-2 B.1.1.529 (Omicron) variant became predominant in the United States by late December 2021, leading to a surge in COVID-19 cases and associated ED visits and hospitalizations. What is added by this report? Despite Omicron seeing the highest reported numbers of COVID-19 cases and hospitalizations during the pandemic, disease severity indicators, including length of stay, ICU admission, and death, were lower than during previous pandemic peaks. What are the implications for public health practice? Although disease severity appears lower with the Omicron variant, the high volume of hospitalizations can strain local health care systems and the average daily number of deaths remains substantial. This underscores the importance of national emergency preparedness, specifically, hospital surge capacity and the ability to adequately staff local health care systems. In addition, being up to date on vaccinations and following other recommended prevention strategies are critical to preventing infections, severe illness, or death from COVID-19. [Description provided by NIOSH]
-
Subjects:
-
Keywords:
-
Source:MMWR 2022 Jan; 71(4):146-152
-
Series:
-
DOI:
-
ISSN:0149-2195
-
Pubmed ID:35085225
-
Pubmed Central ID:PMC9351529
-
Document Type:
-
Genre:
-
Place as Subject:Georgia ; Maryland ; New Jersey ; OSHA Region 2 ; OSHA Region 3 ; OSHA Region 4 ; Pennsylvania ; Virginia
-
CIO:
-
Division:
-
Topic:
-
Location:
-
Pages in Document:7 pdf pages
-
Contributor:Devies, Jourdan ; Gates, Abigail ; Huang, Jay ; Jonson, Heather ; Krawiz, Marc ; Yu, Kalvin
-
Volume:71
-
Issue:4
-
NIOSHTIC Number:nn:20064427
-
Contact Point Address:A. Danielle Iuliano, CDC COVID-19 Emergency Response Team, Atlanta, GA
-
Email:aiuliano@cdc.gov
-
Federal Fiscal Year:2022
-
Peer Reviewed:False
-
Collection(s):
-
Main Document Checksum:urn:sha-512:65a06f75fddecc38c5c5f0b0644153c32ccf01dde43baab123b13f7df6c32d1276c35537387a0dbce1401e2a7d89df4064b80c74e7cc8a45f758d18ddd625459
-
Download URL:
-
File Type:
 [PDF
- 523.89 KB
]
[PDF
- 523.89 KB
]
Supporting Files

File Language:
English

{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like