Efficacy of Dental Evacuation Systems for Aerosol Exposure Mitigation in Dental Clinic Settings
Supporting Files

-
2022/05/01
-
File Language:
English
Details
-
Journal Article:Journal of Occupational and Environmental Hygiene
-
Personal Author:
-
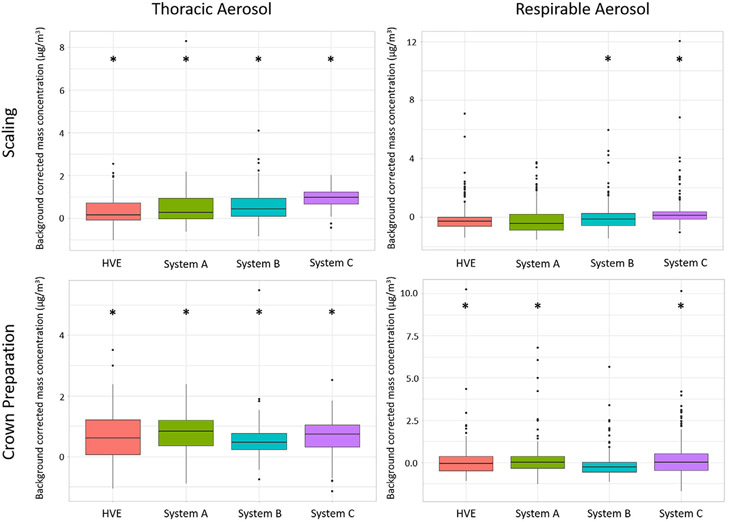
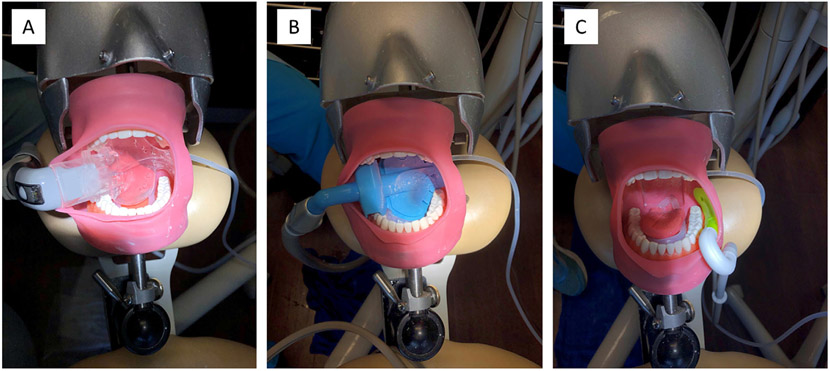
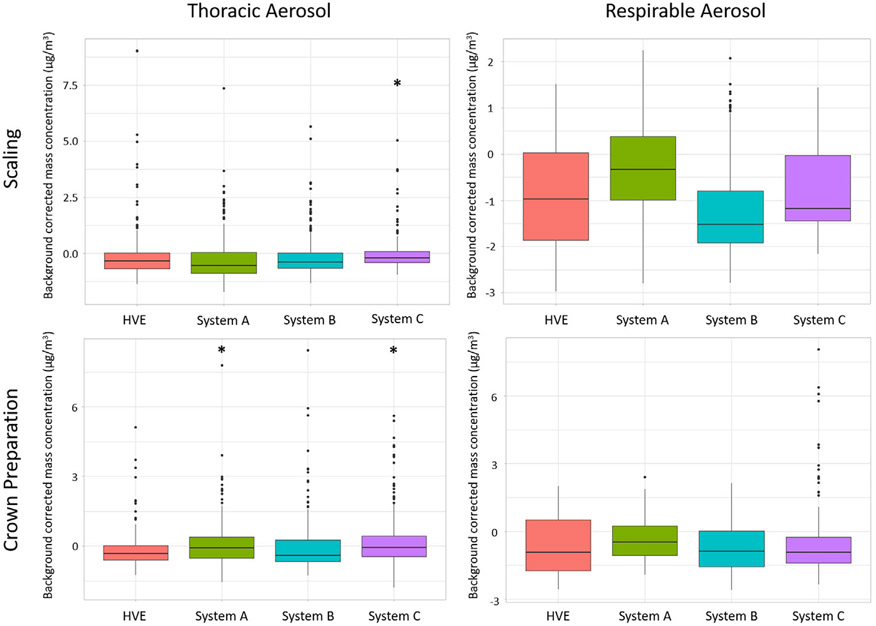
Description:Dental personnel are ranked among the highest risk occupations for exposure to SARS-CoV-2 due to their close proximity to the patient's mouth and many aerosol generating procedures encountered in dental practice. One method to reduce aerosols in dental settings is the use of intraoral evacuation systems. Intraoral evacuation systems are placed directly into a patient's mouth and maintain a dry field during procedures by capturing liquid and aerosols. Although multiple intraoral dental evacuation systems are commercially available, the efficacy of these systems is not well understood. The objectives of this study were to evaluate the efficacy of four dental evacuation systems at mitigating aerosol exposures during simulated ultrasonic scaling and crown preparation procedures. We conducted real-time respirable (PM4) and thoracic (PM10) aerosol sampling during ultrasonic scaling and crown preparation procedures while using four commercially available evacuation systems: a high-volume evacuator (HVE) and three alternative intraoral systems (A, B, C). Four trials were conducted for each system. Respirable and thoracic mass concentrations were measured during procedures at three locations including (1) near the breathing zone (BZ) of the dentist, (2) edge of the dental operatory room approximately 0.9 m away from the mannequin mouth, and (3) hallway supply cabinet located approximately 1.5 m away from the mannequin mouth. Respirable and thoracic mass concentrations measured during each procedure were compared with background concentrations measured in each respective location. Use of System A or HVE reduced thoracic (System A) and respirable (HVE) mass concentrations near the dentist's BZ to median background concentrations most often during the ultrasonic scaling procedure. During the crown preparation, use of System B or HVE reduced thoracic (System B) and respirable (HVE or System B) near the dentist's BZ to median background concentrations most often. Although some differences in efficacy were noted during each procedure and aerosol size fraction, the difference in median mass concentrations among evacuation systems was minimal, ranging from 0.01 to 1.48 µg/m3 across both procedures and aerosol size fractions. [Description provided by NIOSH]
-
Subjects:
-
Keywords:
-
Source:J Occup Environ Hyg 2022 May; 19(5):281-294
-
ISSN:1545-9624
-
Pubmed ID:35289720
-
Pubmed Central ID:PMC9365099
-
Document Type:
-
Funding:
-
Genre:
-
Place as Subject:
-
CIO:
-
Division:
-
Topic:
-
Location:
-
Pages in Document:22 pdf pages
-
Volume:19
-
Issue:5
-
NIOSHTIC Number:nn:20065244
-
Contact Point Address:Brie Hawley Blackley, Respiratory Health Division, National Institute for Occupational Safety and Health, Morgantown, WV, USA
-
Email:Ygd2@cdc.gov
-
Federal Fiscal Year:2022
-
NORA Priority Area:
-
Peer Reviewed:True
-
Collection(s):
-
Main Document Checksum:urn:sha-512:f31ad45b63ff4ec04d7e0f7aeb91bd536c5d9b53aba043e6619dada6b334448bcf07b2345151078d3578add4211378107c684c66734a7b74d9fc6050f915c63b
-
Download URL:
-
File Type:
 [PDF
- 1.01 MB
]
[PDF
- 1.01 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like