Health impact and cost-effectiveness of HIV testing, linkage, and early antiretroviral treatment in the Botswana Combination Prevention Project
Supporting Files

-
8 01 2022
-
File Language:
English
Details
-
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:Resch, Stephen C. ; Foote, Julia H. A. ; Wirth, Kathleen E. ; Lasry, Arielle ; Scott, Justine A. ; Moore, Janet ; Shebl, Fatma M. ; Gaolathe, Tendani ; Feser, Mary K. ; Lebelonyane, Refeletswe ; Hyle, Emily P. ; Mmalane, Mompati O. ; Bachanas, Pamela ; Yu, Liyang ; Makhema, Joseph M. ; Holme, Molly Pretorius ; Essex, Max ; Alwano, Mary Grace ; Lockman, Shahin ; Freedberg, Kenneth A.
-
Description:Background:
The Botswana Combination Prevention Project tested the impact of combination prevention (CP) on HIV incidence in a community-randomized trial. Each trial arm had ~55,000 people, 26% HIV prevalence, and 72% baseline ART coverage. Results showed intensive testing and linkage campaigns, expanded antiretroviral treatment (ART), and voluntary male medical circumcision (VMMC) referrals increased coverage and decreased incidence over ~29 months follow-up. We projected lifetime clinical impact and cost-effectiveness of CP in this population.
Setting:
Rural and peri-urban communities in Botswana.
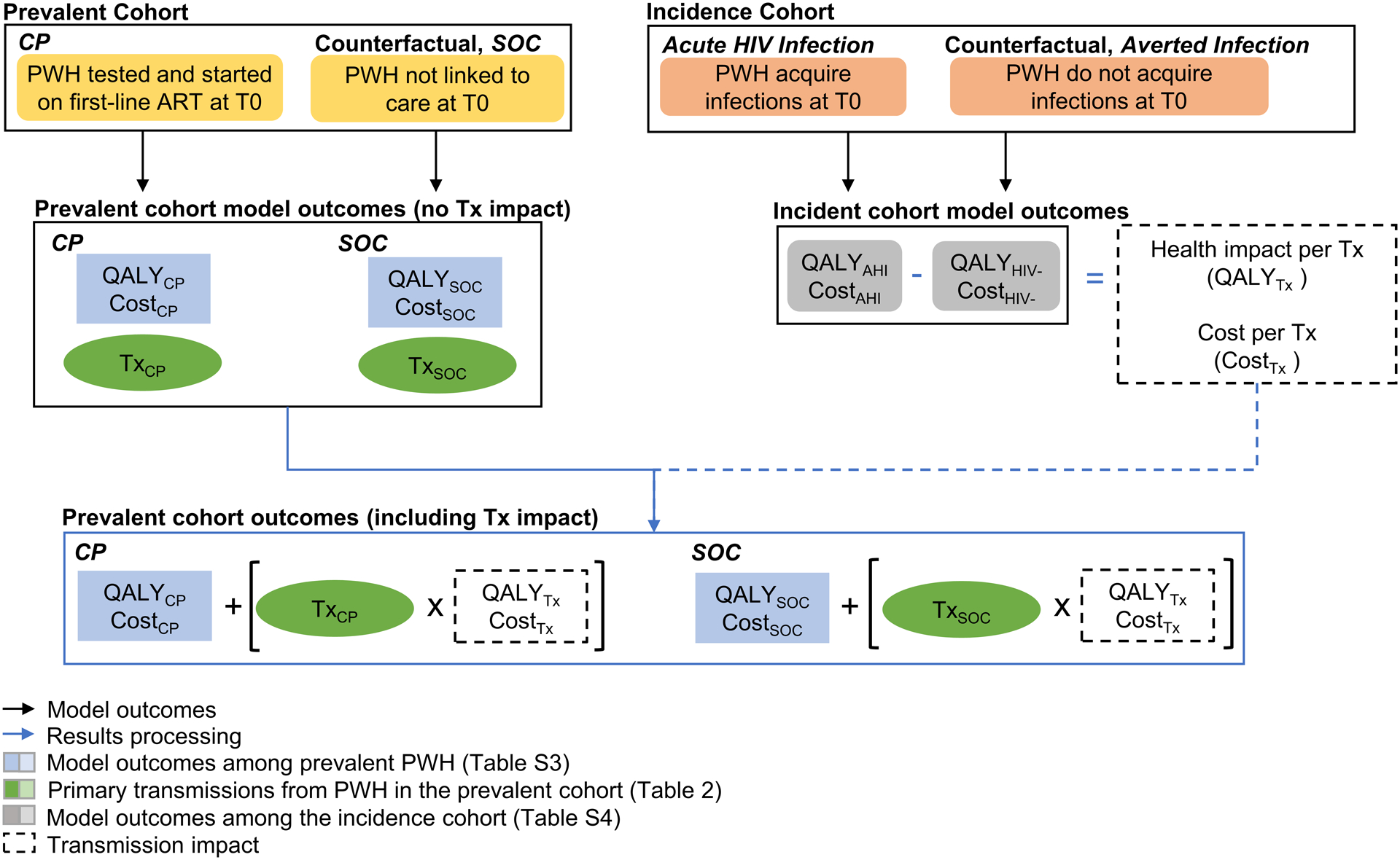
Methods:
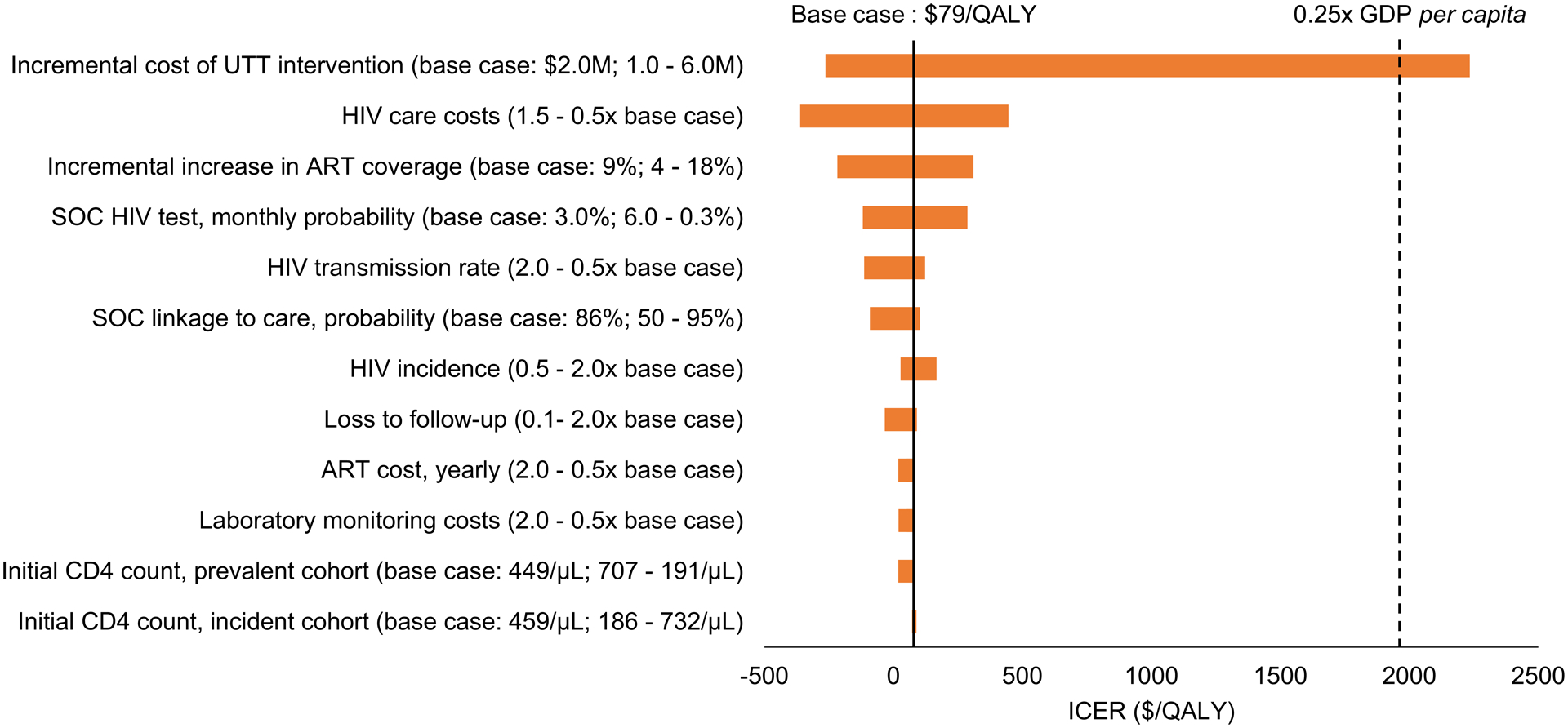
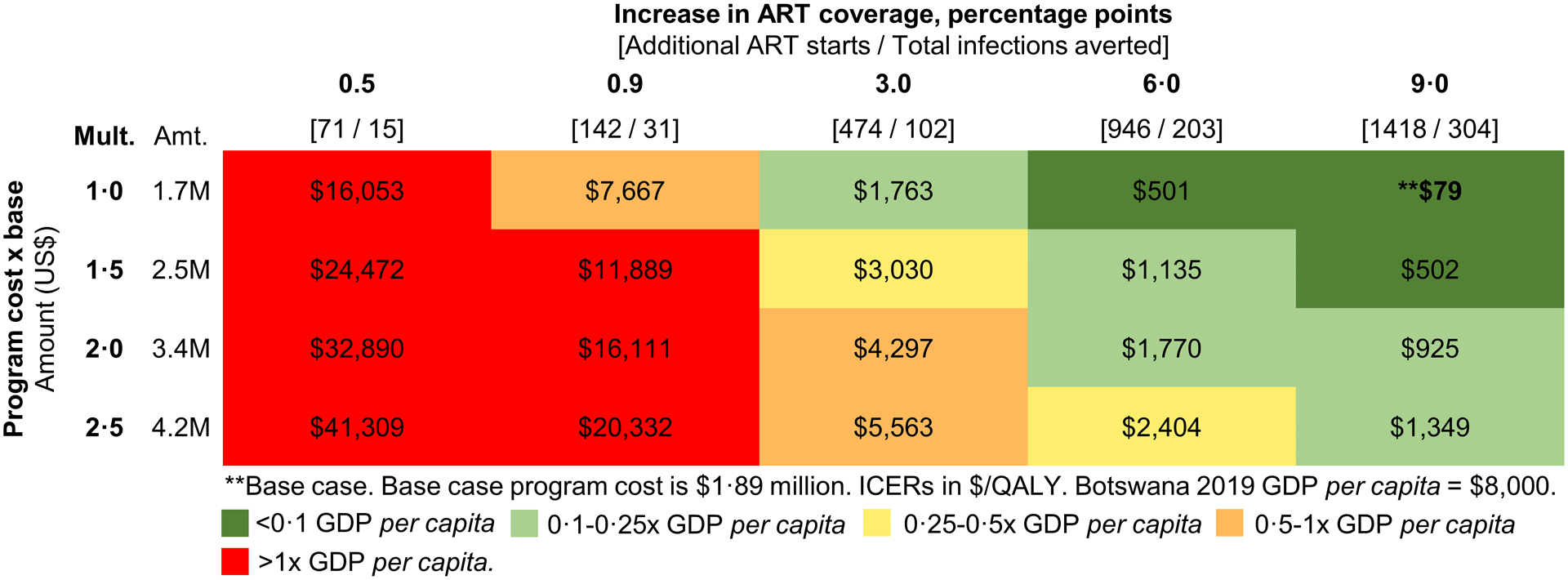
We used the Cost-Effectiveness of Preventing AIDS Complications (CEPAC) model to estimate lifetime health impact and cost of 1) earlier ART initiation, and 2) averting an HIV infection, which we applied to incremental ART initiations and averted infections calculated from trial data. We determined the incremental cost-effectiveness ratio (ICER, US$/QALY) for CP vs. standard of care.
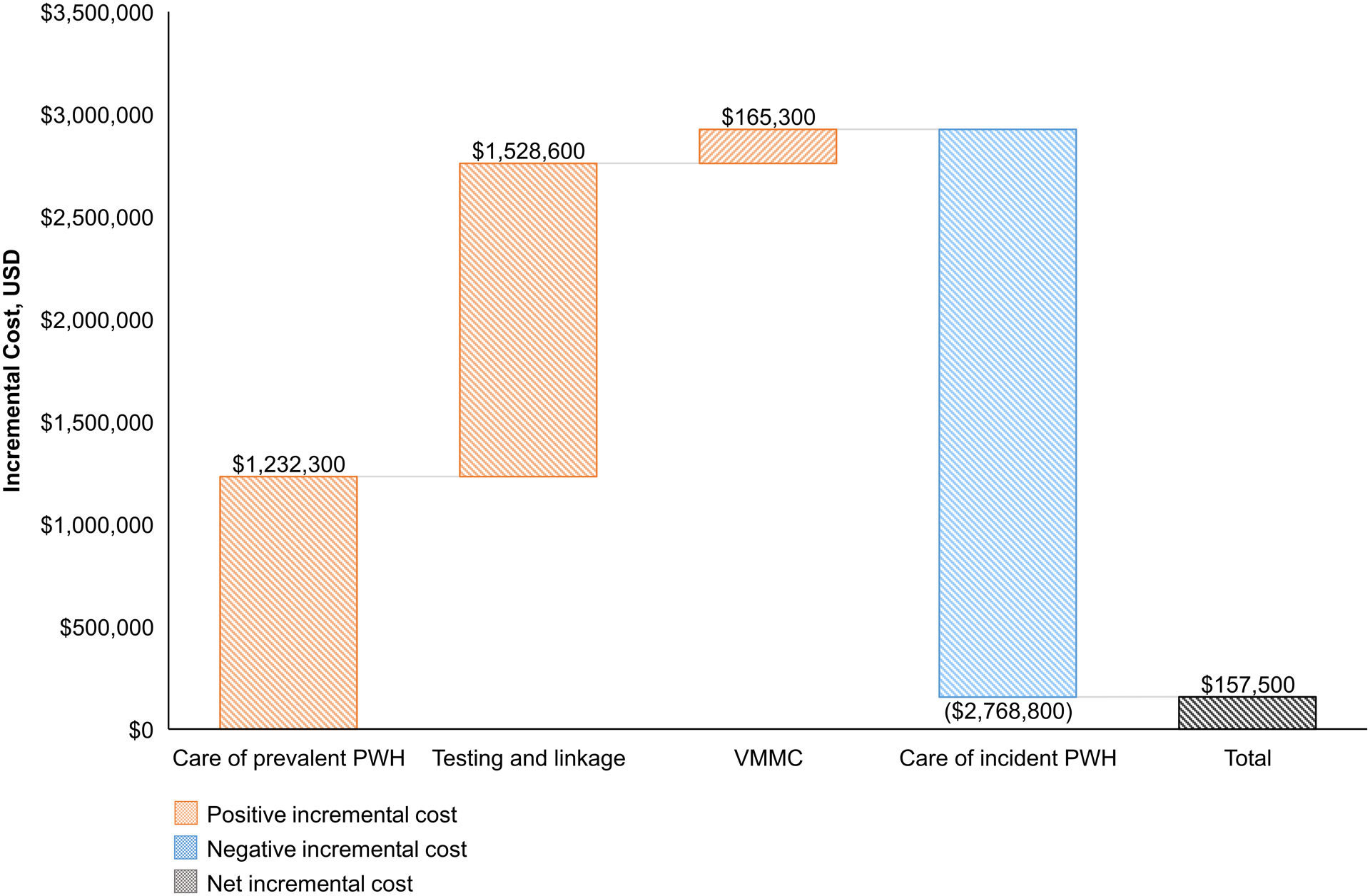
Results:
In CP, 1,418 additional people with HIV initiated ART and an additional 304 infections were averted. For each additional person started on ART, life expectancy increased 0.90 QALYs and care costs increased by $869. For each infection averted, life expectancy increased 2.43 QALYs with $9,200 in care costs saved. With CP, an additional $1.7 million were spent on prevention and $1.2 million on earlier treatment. These costs were mostly offset by decreased care costs from averted infections, resulting in an ICER of $79 per QALY.
Conclusions:
Enhanced HIV testing, linkage, and early ART initiation improves life expectancy, reduces transmission, and can be cost-effective or cost-saving in settings like Botswana.
-
Subjects:
-
Source:J Acquir Immune Defic Syndr. 90(4):399-407
-
Pubmed ID:35420554
-
Pubmed Central ID:PMC9295776
-
Document Type:
-
Funding:CC999999/ImCDC/Intramural CDC HHSUnited States/ ; K01 HL123349/HL/NHLBI NIH HHSUnited States/ ; R37 AI058736/AI/NIAID NIH HHSUnited States/ ; K24 AI131928/AI/NIAID NIH HHSUnited States/ ; R37 AI051164/AI/NIAID NIH HHSUnited States/ ; U01 GH000447/GH/CGH CDC HHSUnited States/ ; U2G GH001911/GH/CGH CDC HHSUnited States/ ; PEPFAR/PEPFARUnited States/
-
Volume:90
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:a68df3980e5af7266633147ab8f962acd4766546d22f8f48213cfe2cbc1c61a2
-
Download URL:
-
File Type:
 [PDF
- 1.02 MB
]
[PDF
- 1.02 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access