Trends and practices for managing low-risk prostate cancer: a SEER-Medicare study
Supporting Files

-
3-2022
-
File Language:
English
Details
-
Alternative Title:Prostate Cancer Prostatic Dis
-
Personal Author:
-
Description:Background
Expectant management (EM) has been widely recommended for men with low-risk prostate cancers (PCa). We evaluated trends in EM and the sociodemographic and clinical factors associated with EM, initiating a National Comprehensive Cancer Network guideline-concordant active surveillance (AS) monitoring protocol, and switching from EM to active treatment (AT).
Methods
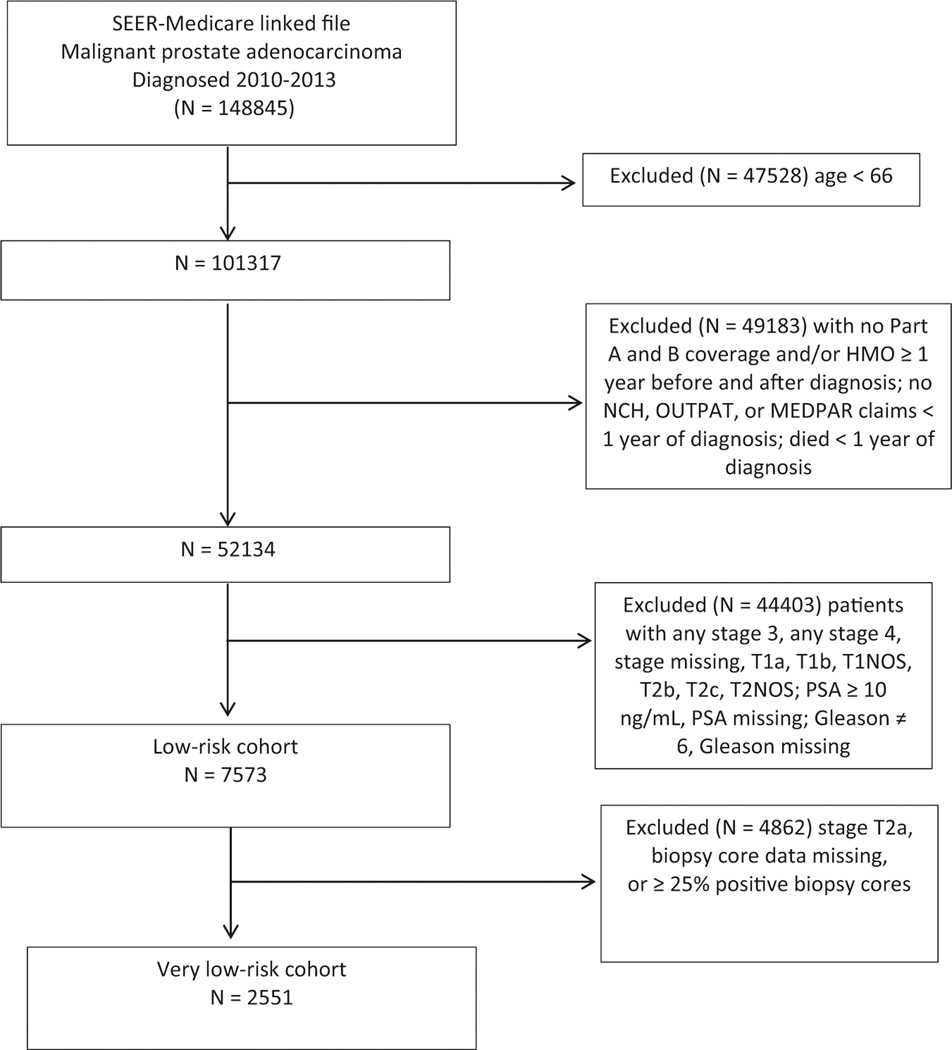
We used the SEER-Medicare database to identify men ages 66+ diagnosed with a low-risk PCa (PSA < 10 ng/mL, Gleason ≤ 6, stage ≤ T2a) in 2010–2013 with ≥1 year of follow-up. We used claims data to capture (1) PCa treatments, including surgical procedures, radiotherapy, and hormone therapy, and (2) AS monitoring procedures, including PSA tests and prostate biopsy. We defined EM as receiving no AT within 1 year of diagnosis. We used multivariable regression techniques to identify factors associated with EM, initiating AS monitoring, and switching to AT.
Results
During the study period, EM increased from 29.4% to 49.0%, p < 0.01. Age < 77, being married/partnered, non-Hispanic ethnicity, higher median ZIP code income, lower PSA levels, stage T1c, and more recent year of diagnosis were associated with EM. Nearly 39% of the EM cohort initiated AS monitoring; age <77, White race, being married/partnered, higher median ZIP code income, and lower PSA levels were associated with initiating AS. By three years after diagnosis, 21.3% of the EM cohort had switched to AT, usually after undergoing AS monitoring procedures.
Discussion
We found increasing uptake of EM over time, though over 50% still received AT. About 60% of EM patients did not initiate AS monitoring, even among those with life expectancy >10 years, implying that a substantial proportion was being managed by watchful waiting. AS monitoring was associated with switching to AT, suggesting that treatment decisions likely were based on cancer progression.
-
Subjects:
-
Source:Prostate Cancer Prostatic Dis. 25(1):100-108
-
Pubmed ID:34108645
-
Pubmed Central ID:PMC8976291
-
Document Type:
-
Funding:
-
Volume:25
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha256:d1a59a6662c27d7f2f727d04f0d1979584b5900452b690084cd00fdce068b6a0
-
Download URL:
-
File Type:
 [PDF
- 427.12 KB
]
[PDF
- 427.12 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access