Multimodal Analgesia Reduces Opioid Requirements in Trauma Patients with Rib Fractures
Supporting Files

-
3-01-
-
File Language:
English
Details
-
Alternative Title:J Trauma Acute Care Surg
-
Personal Author:
-
Corporate Authors:
-
Description:Background:
Rib fractures are common in trauma patients and are associated with significant morbidity and mortality. Adequate analgesia is essential to avoid the complications associated with rib fractures. Opioids are frequently used for analgesia in these patients. This study compared the effect of a multimodal pain regimen (MMPR) on inpatient opioid use and outpatient opioid prescribing practices in adult trauma patients with rib fractures.
Study Design:
A pre-post cohort study of adult trauma patients with rib fractures was conducted at a Level 1 trauma center before (PRE) and after (POST) implementation of an MMPR. Control charts were utilized to assess changes over time. Patients on long-acting opioids before admission and those on continuous opioid infusions were excluded. Primary outcomes were oral opioid administration during the first 5 days of hospitalization and opioids prescribed at discharge. Opioid data were converted to morphine milligram equivalents (MME).
Results:
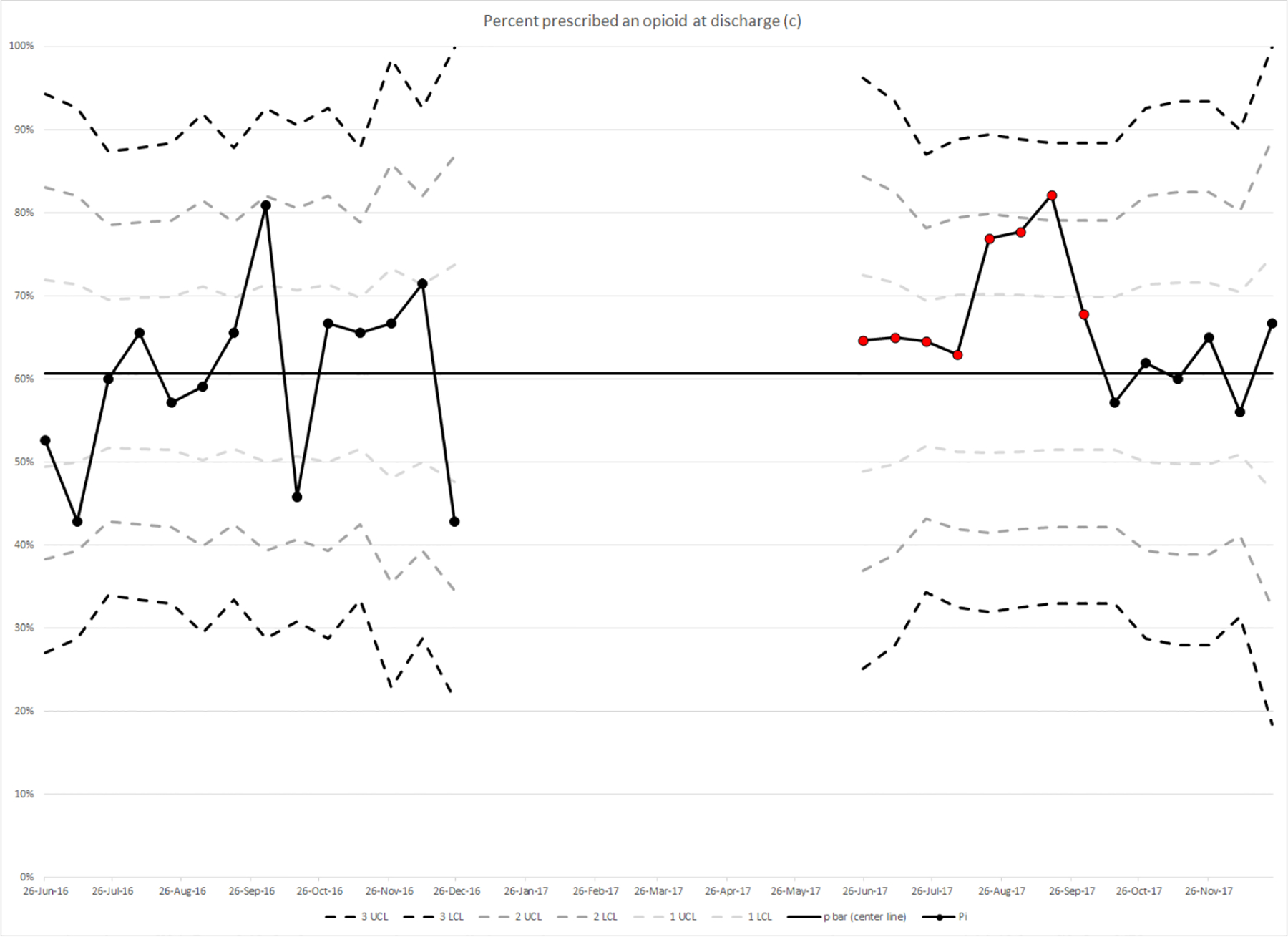
653 patients met inclusion criteria (323 PRE, 330 POST). There was a significant reduction in the daily MME during the second through fifth days of hospitalization; and the average inpatient MME over the first 5 inpatient days (23 MME PRE vs. 17 MME POST, p=0.0087). There was a significant reduction in the total outpatient MME prescribed upon discharge (322 MME PRE vs. 225 MME POST, p=0.006). There was evidence for special cause variation in percent of gabapentanoid prescribed (higher POST), average MME while in the hospital (lower POST), and the percent of patients prescribed an opioid at discharge (higher POST). There was no special cause variation related to percent of patients receiving opioids in the hospital.
Conclusion:
The implementation of an MMPR in patients with rib fractures resulted in significant reduction in inpatient opioid consumption and was associated with a reduction in the quantity of opiates prescribed at discharge.
Level of Evidence
Level IV Retrospective comparison
-
Subjects:
-
Source:J Trauma Acute Care Surg. 92(3):588-596
-
Pubmed ID:34882599
-
Pubmed Central ID:PMC8866226
-
Document Type:
-
Funding:
-
Volume:92
-
Issue:3
-
Collection(s):
-
Main Document Checksum:urn:sha256:7e5ae49239a9d97937934c0991e2f9164eac1a48d22b579a34e4d9c7441b378a
-
Download URL:
-
File Type:
 [PDF
- 1.04 MB
]
[PDF
- 1.04 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access