In-Person vs Electronic Directly Observed Therapy for Tuberculosis Treatment Adherence
Supporting Files

-
1 20 2022
-
File Language:
English
Details
-
Alternative Title:JAMA Netw Open
-
Personal Author:
-
Corporate Authors:
-
Description:IMPORTANCE
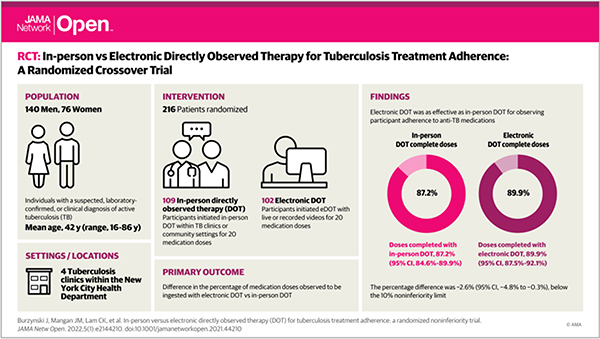
Electronic directly observed therapy (DOT) is used increasingly as an alternative to in-person DOT for monitoring tuberculosis treatment. Evidence supporting its efficacy is limited.
OBJECTIVE
To determine whether electronic DOT can attain a level of treatment observation as favorable as in-person DOT.
DESIGN, SETTING, AND PARTICIPANTS
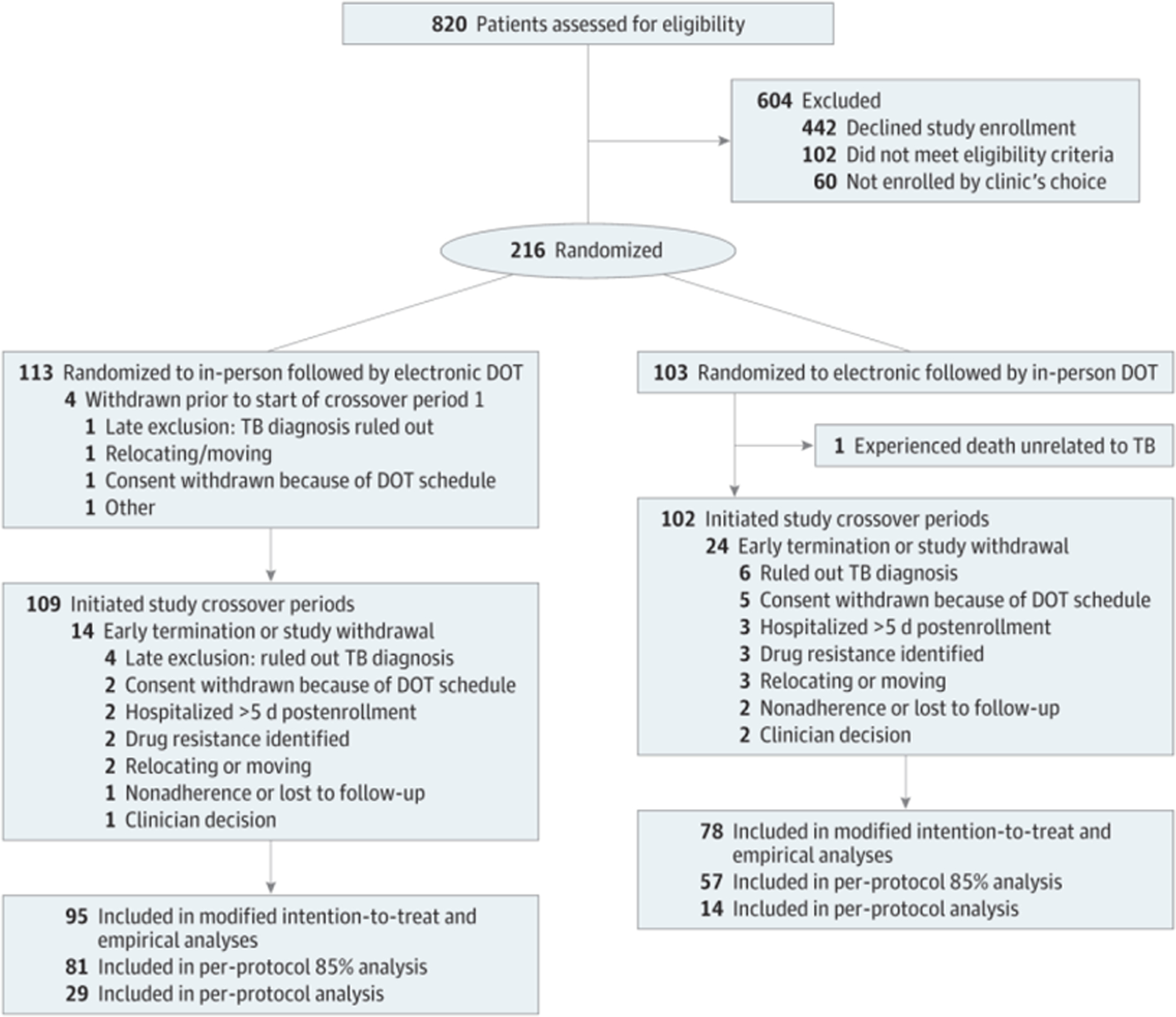
This was a 2-period crossover, noninferiority trial with initial randomization to electronic or in-person DOT at the time outpatient tuberculosis treatment began. The trial enrolled 216 participants with physician-suspected or bacteriologically confirmed tuberculosis from July 2017 to October 2019 in 4 clinics operated by the New York City Health Department. Data analysis was conducted between March 2020 and April 2021.
INTERVENTIONS
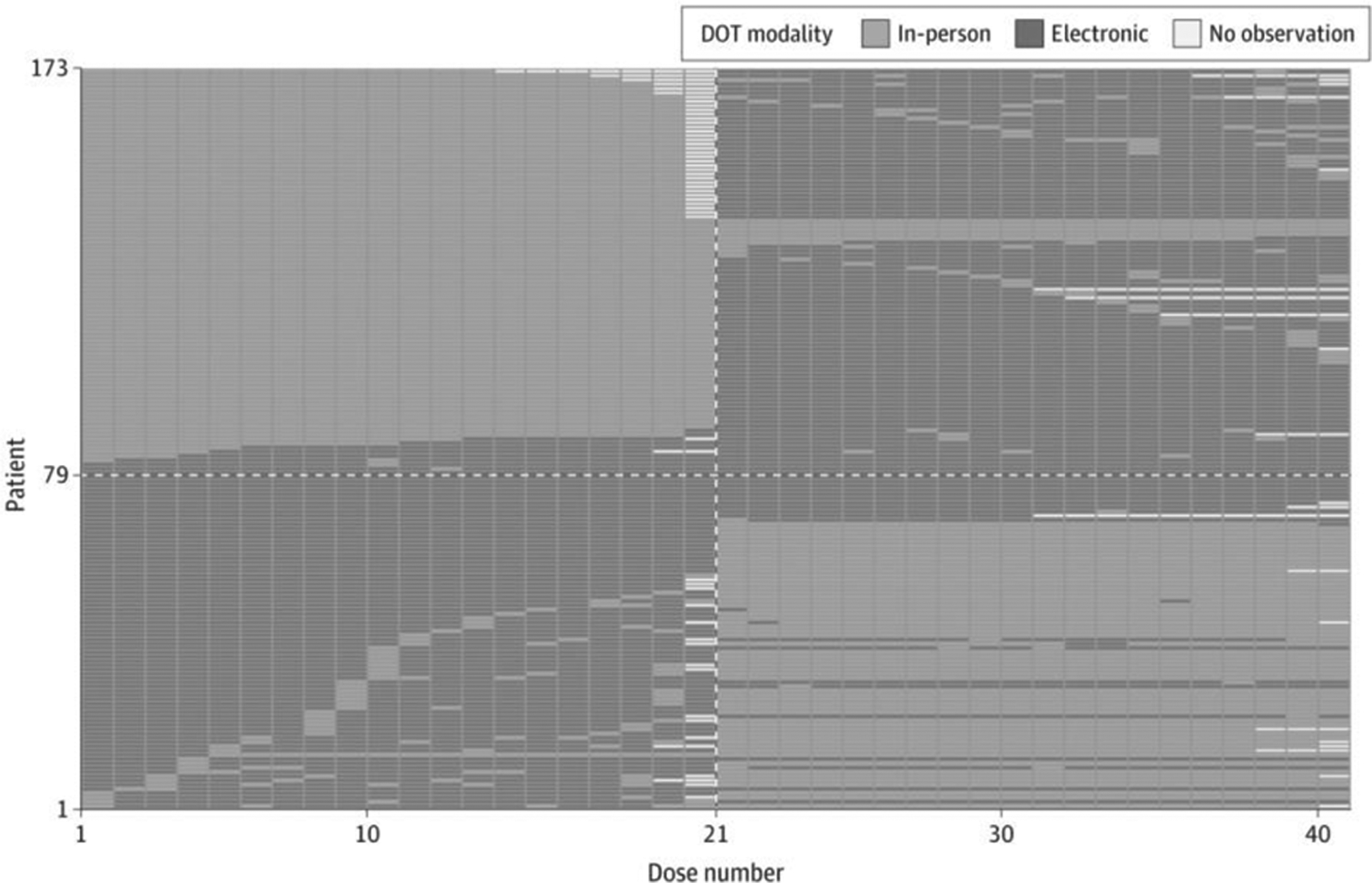
Participants were asked to complete 20 medication doses using 1 DOT method, then switched methods for another 20 doses. With in-person therapy, participants chose clinic or community-based DOT; with electronic DOT, participants chose live video-conferencing or recorded videos.
MAIN OUTCOMES AND MEASURES
Difference between the percentage of medication doses participants were observed to completely ingest with in-person DOT and with electronic DOT. Noninferiority was demonstrated if the upper 95% confidence limit of the difference was 10% or less. We estimated the percentage of completed doses using a logistic mixed effects model, run in 4 modes: modified intention-to-treat, per-protocol, per-protocol with 85% or more of doses conforming to the randomization assignment, and empirical. Confidence intervals were estimated by bootstrapping (with 1000 replicates).
RESULTS
There were 173 participants in each crossover period (median age, 40 years [range, 16–86 years]; 140 [66%] men; 80 [37%] Asian and Pacific Islander, 43 [20%] Black, and 71 [33%] Hispanic individuals) evaluated with the model in the modified intention-to-treat analytic mode. The percentage of completed doses with in-person DOT was 87.2% (95% CI, 84.6%–89.9%) vs 89.8% (95% CI, 87.5%–92.1%) with electronic DOT. The percentage difference was −2.6% (95% CI, −4.8% to −0.3%), consistent with a conclusion of noninferiority. The 3 other analytic modes yielded equivalent conclusions, with percentage differences ranging from −4.9% to −1.9%.
CONCLUSIONS AND RELEVANCE
In this trial, the percentage of completed doses under electronic DOT was noninferior to that under in-person DOT. This trial provides evidence supporting the efficacy of this digital adherence technology, and for the inclusion of electronic DOT in the standard of care.
TRIAL REGISTRATION
ClinicalTrials.gov Identifier: NCT03266003
-
Subjects:
-
Source:JAMA Netw Open. 5(1):e2144210
-
Pubmed ID:35050357
-
Pubmed Central ID:PMC8777548
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:5
-
Issue:1
-
Collection(s):
-
Main Document Checksum:urn:sha256:f2d8f910d2a0ac3df0671fc2c57c993f2ab4fbbad183cfefb6b76d1e29fc0afd
-
Download URL:
-
File Type:
 [PDF
- 732.51 KB
]
[PDF
- 732.51 KB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access