Impact of Timing of Antiretroviral Treatment and Birth Weight on Mother-to-Child Human Immunodeficiency Virus Transmission: Findings From an 18-Month Prospective Cohort of a Nationally Representative Sample of Mother–Infant Pairs During the Transition From Option A to Option B+ in Zimbabwe
Supporting Files

-
2 01 2018
-
File Language:
English
Details
-
Alternative Title:Clin Infect Dis
-
Personal Author:
-
Description:Background.
Preventing mother-to-child transmission of human immunodeficiency virus transmission (MTCT) depends on early initiation of antiretroviral therapy (ART). We report the 18-month MTCT risk during the transition from Option A to Option B+ in Zimbabwe, and assess whether ART preconception could eliminate MTCT in breastfeeding populations.
Methods.
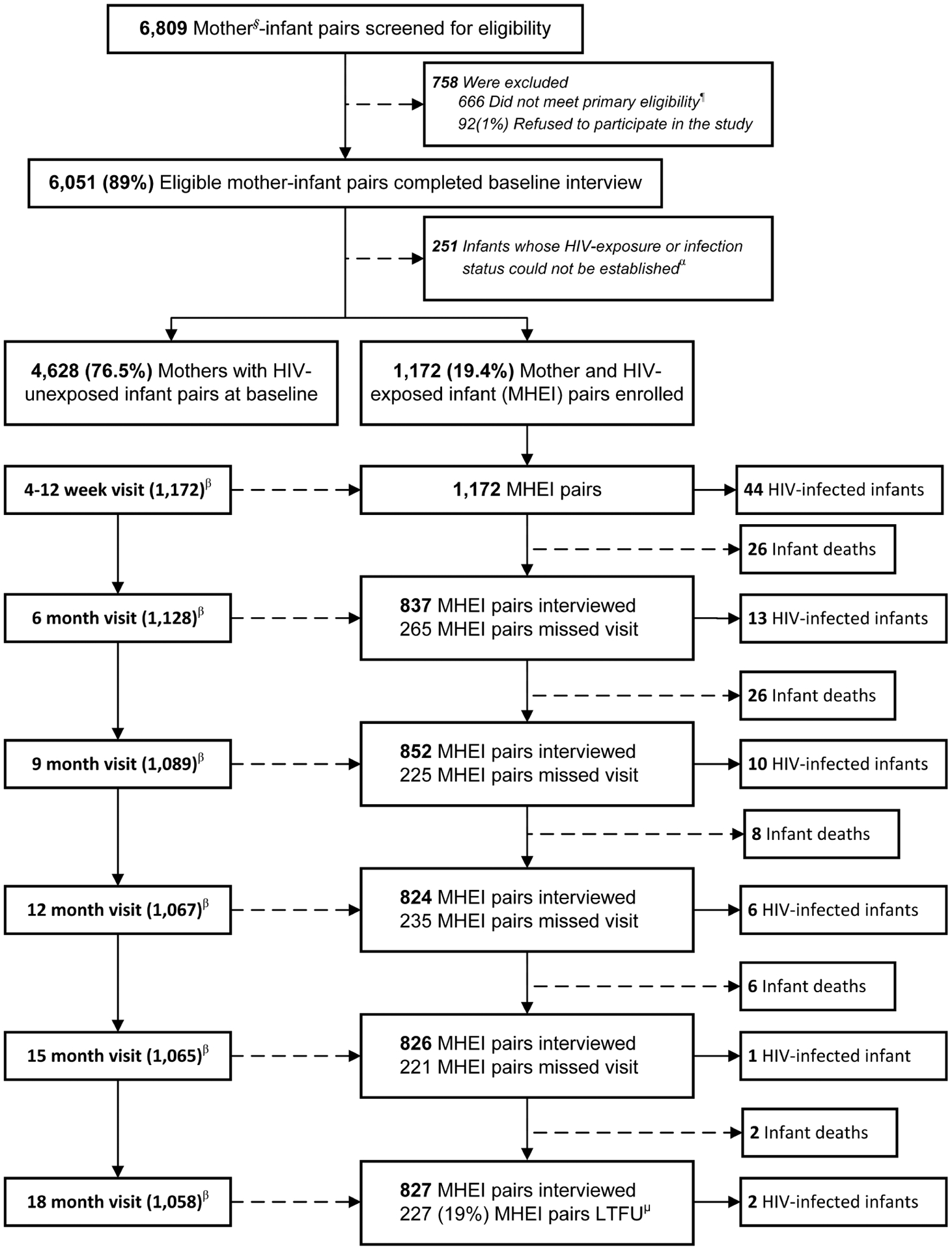
In 2013, we consecutively recruited a nationally representative sample of 6051 infants aged 4–12 weeks and their mothers from 151 immunization clinics using a multistage stratified cluster sampling method. We identified 1172 human immunodeficiency virus (HIV)–exposed infants and evaluated them at baseline and every 3 months until the child became HIV-infected, died, or reached age 18 months.
Results.
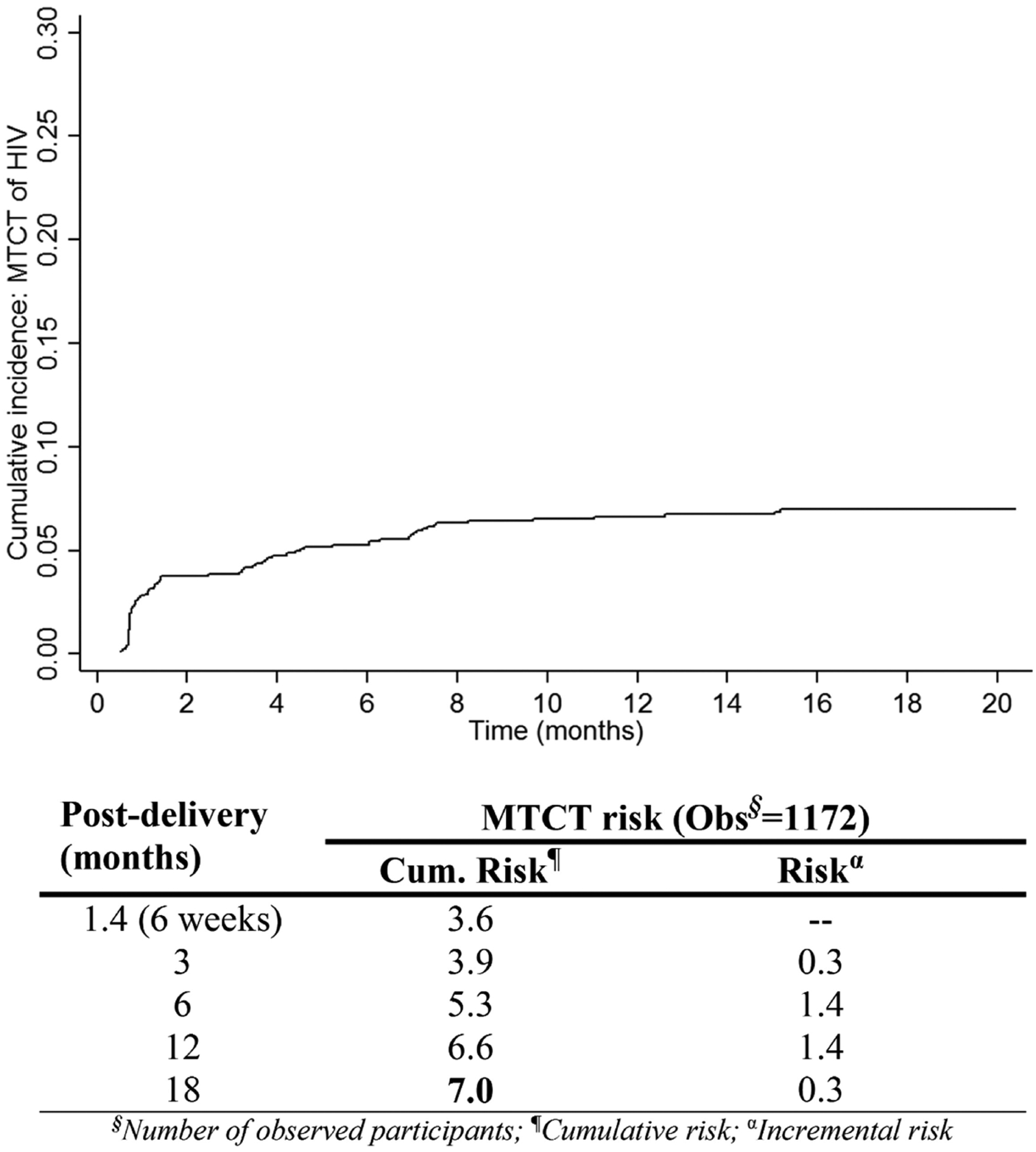
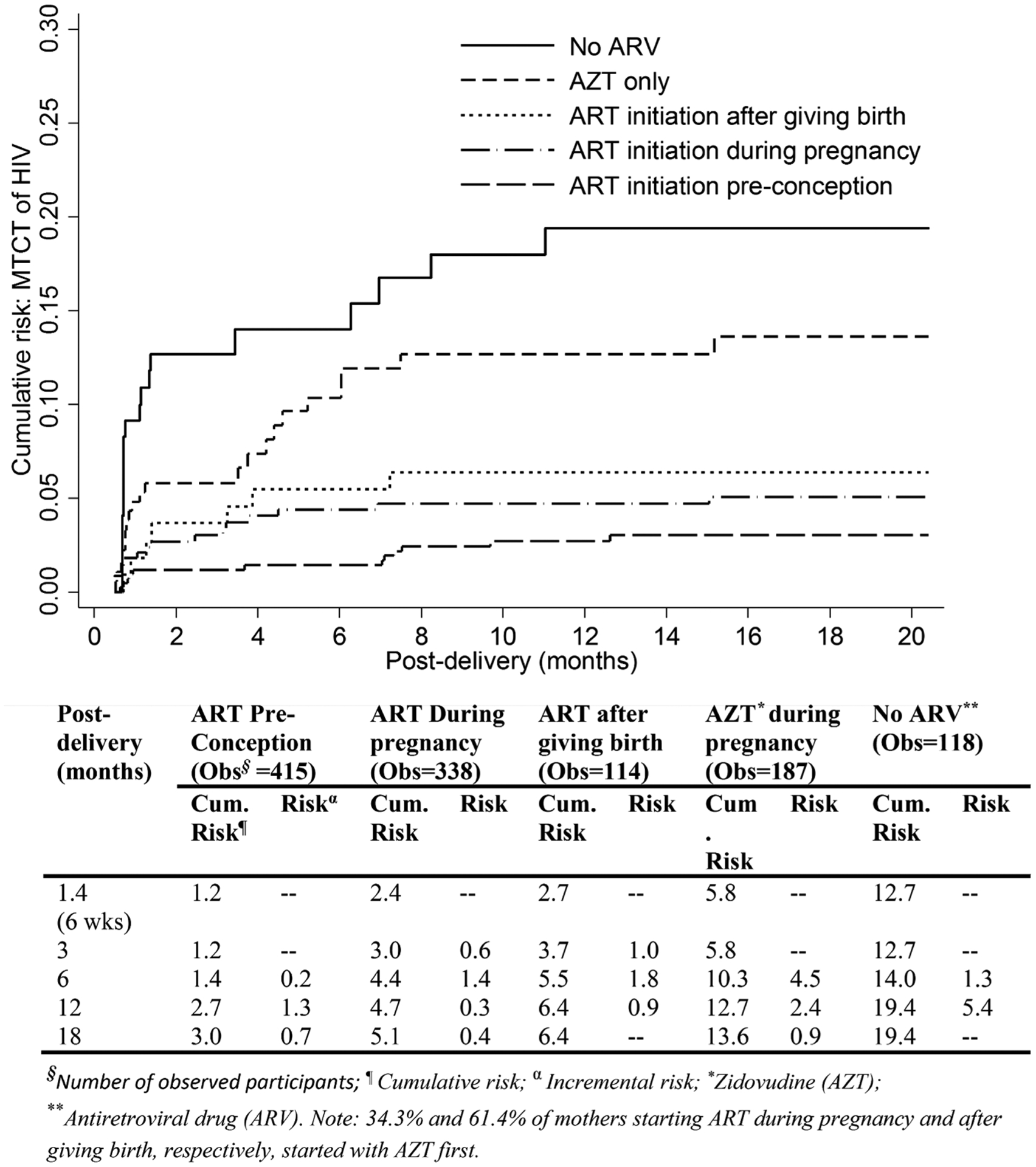
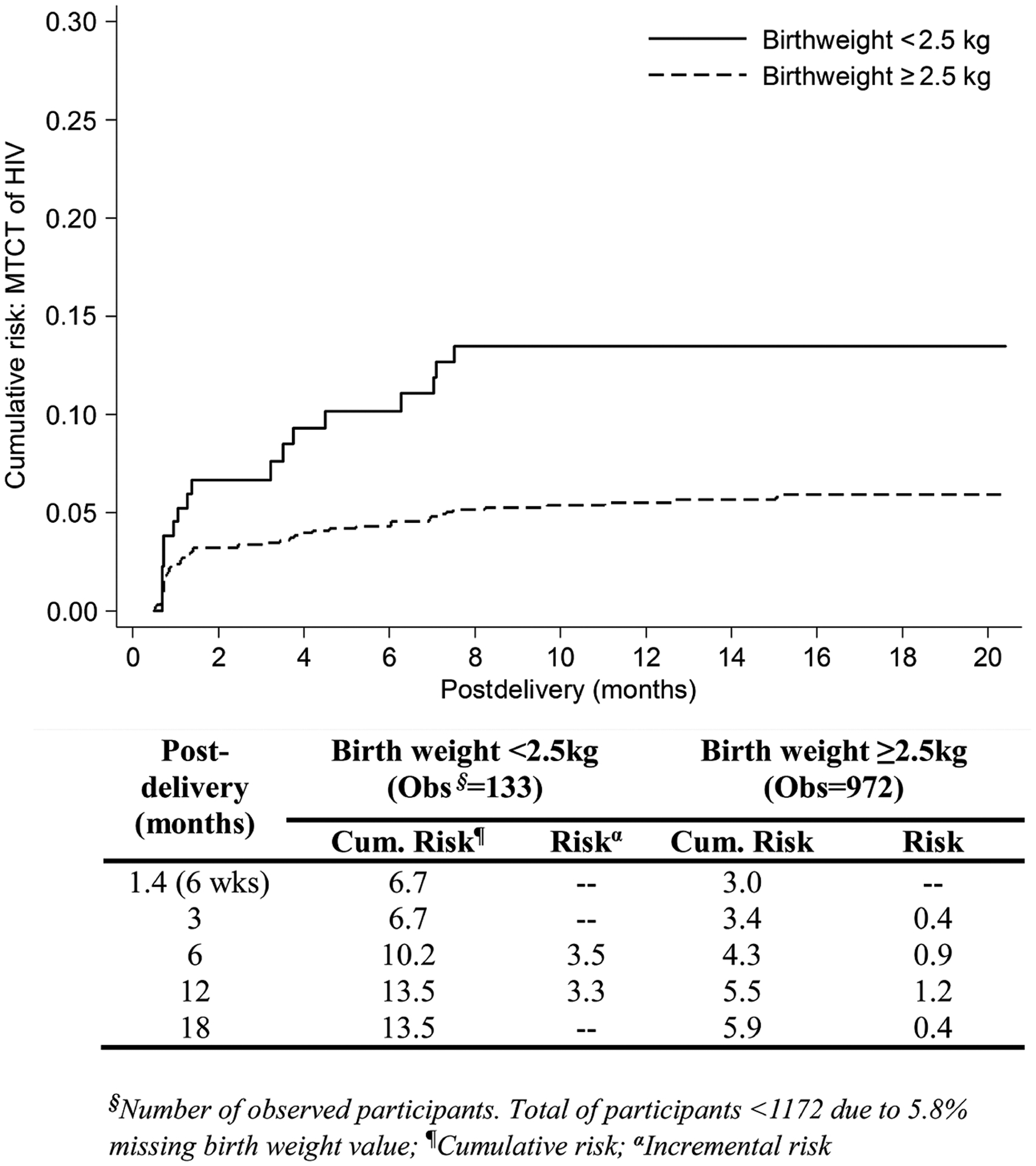
The cumulative MTCT risk through 18 months postdelivery was 7.0%. Of the HIV-infected mothers, 35.3% started ART preconception, 28.9% during pregnancy, and 9.7% after delivery, and 16.0% received zidovudine during pregnancy. Compared to mothers without antiretroviral drug use, MTCT among those starting ART preconception and during pregnancy was lower by 88% (adjusted hazard ratio [aHR], 0.12; 95% confidence interval [CI], .06–.24) and 75% (aHR, 0.25; 95% CI, .14–.45), respectively. HIV-exposed infants with birth weight <2.5 kg (low birth weight) were 2.6-fold more likely to acquire HIV infection compared to those with birth weight ≥2.5 kg (aHR, 2.57; 95% CI, 1.44–4.59). Controlling for other factors, breastfeeding was not significantly associated with MTCT.
Conclusions.
ART preconception has the highest impact on reducing MTCT, indicating that HIV-infected, reproductive-age women should be prioritized in “treat-all” strategies. HIV-infected mothers without ART use should be identified at the first immunization visit and treatment initiated to reduce postdelivery MTCT. MTCT risk is higher in mothers with low-birth-weight deliveries.
-
Subjects:
-
Source:Clin Infect Dis. 66(4):576-585
-
Pubmed ID:29401270
-
Pubmed Central ID:PMC8764936
-
Document Type:
-
Funding:
-
Place as Subject:
-
Volume:66
-
Issue:4
-
Collection(s):
-
Main Document Checksum:urn:sha256:cd158a9e8af262e898f2f74f7ec414c75c413965d1c9d596e30279b57666b6e4
-
Download URL:
-
File Type:
 [PDF
- 1.10 MB
]
[PDF
- 1.10 MB
]
Supporting Files

File Language:
English
ON THIS PAGE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
CDC Public Access