Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, March 2021 / Vol. 70 / No. SS-2
Supporting Files
Public Domain

-
March 19, 2021
File Language:
English
Details
-
Alternative Title:Malaria Surveillance — U.S. 2017
-
Journal Article:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries
-
Personal Author:
-
Corporate Authors:
-
Description:Problem/Condition
Malaria in humans is caused by intraerythrocytic protozoa of the genus Plasmodium. These parasites are transmitted by the bite of an infective female Anopheles species mosquito. The majority of malaria infections in the U.S. occur among persons who have traveled to regions with ongoing malaria Transmission. However, malaria is occasionally acquired by persons who have not traveled out of the country through exposure to infected blood products, Congenital Transmission, nosocomial exposure, or local mosquito borne Transmission. Malaria Surveillance in the U.S. is conducted to provide information on its occurrence (e.g., temporal, geographic, and demographic), guide Prevention and treatment Rec. for travelers and patients, and facilitate rapid Transmission control measures if locally acquired cases are identified.
Period Covered
This report summarizes confirmed malaria cases in persons with onset of illness in 2017 and Trends in previous years.
Description of System
Malaria cases diagnosed by blood film microscopy, polymerase chain reaction, or rapid diagnostic tests are reported to local and state health departments through electronic laboratory reports or by health care providers or laboratory staff members. Case investigations are conducted by local and state health departments, and Rep. are transmitted to CDC through the National Malaria Surveillance System (NMSS), the National Notifiable Diseases Surveillance System (NNDSS), or direct CDC consultations. CDC reference laboratories provide diagnostic assistance and conduct antimalarial drug resistance marker testing on blood samples submitted by health care providers or local or state health departments. This report summarizes data from the integration of all cases from NMSS and NNDSS, CDC reference laboratory reports, and CDC clinical consultations.
Results
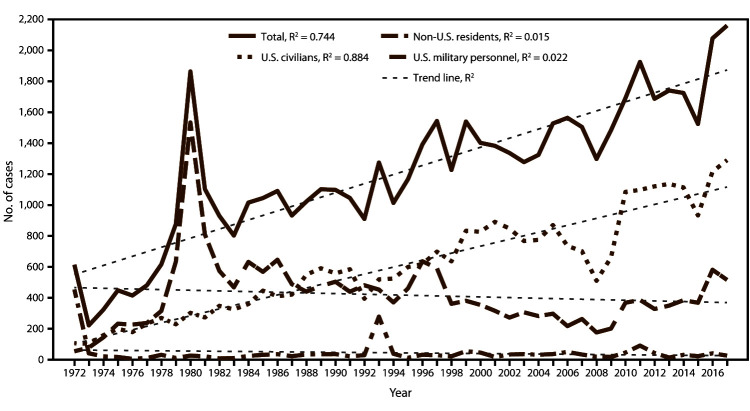
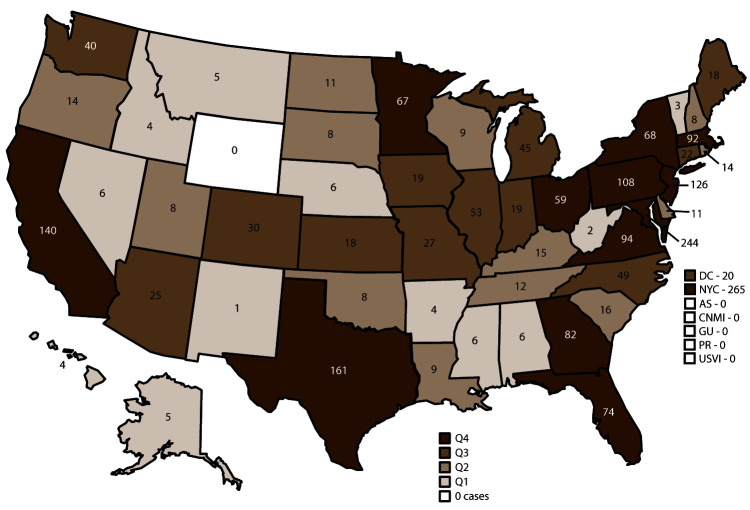
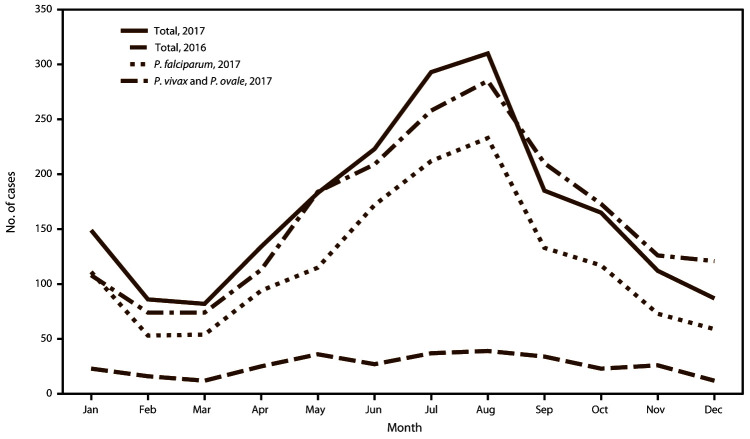
CDC received reports of 2,161 confirmed malaria cases with onset of symptoms in 2017, including two Congenital cases, three cryptic cases, and two cases acquired through blood transfusion. The number of malaria cases diagnosed in the U.S. has been increasing since the mid-1970s; in 2017, the number of cases reported was the highest in 45 years, surpassing the previous peak of 2,078 confirmed cases reported in 2016. Of the cases in 2017, a total of 1,819 (86.1%) were imported cases that originated from Africa; 1,216 (66.9%) of these came from West Africa. The overall proportion of imported cases originating from West Africa was greater in 2017 (57.6%) than in 2016 (51.6%). Among all cases, P. falciparum accounted for the majority of infections (1,523 [70.5%]), followed by P. vivax (216 [10.0%]), P. ovale (119 [5.5%]), and P. malariae (55 [2.6%]). Infections by two or more species accounted for 22 cases (1.0%). The infecting species was not reported or was undetermined in 226 cases (10.5%). CDC provided diagnostic assistance for 9.5% of confirmed cases and tested 8.0% of specimens with P. falciparum infections for antimalarial resistance markers. Most patients (94.8%) had symptom onset <90 days after returning to the U.S. from a country with malaria Transmission. Of the U.S. civilian patients who reported reason for travel, 73.1% were visiting friends and relatives. The proportion of U.S. residents with malaria who reported taking any chemoprophylaxis in 2017 (28.4%) was similar to that in 2016 (26.4%), and adherence was poor among those who took chemoprophylaxis. Among the 996 U.S. residents with malaria for whom information on chemoprophylaxis use and travel region were known, 93.3% did not adhere to or did not take a CDC-recommended chemoprophylaxis regimen. Among 805 women with malaria, 27 reported being pregnant. Of these, 10 pregnant women were U.S. residents, and none reported taking chemoprophylaxis to prevent Malaria A total of 26 (1.2%) malaria cases occurred among U.S. military personnel in 2017, fewer than in 2016 (41 [2.0%]). Among all reported cases in 2017, a total of 312 (14.4%) were classified as severe malaria illnesses, and seven persons died. In 2017, CDC analyzed 117 P. falciparum-positive and six P. falciparum mixed-species samples for antimalarial resistance markers (although certain loci were untestable in some samples); identification of genetic polymorphisms associated with resistance to pyrimethamine were found in 108 (97.3%), to sulfadoxine in 77 (69.4%), to chloroquine in 38 (33.3%), to mefloquine in three (2.7%), and to atovaquone in three (2.7%); no specimens tested contained a marker for artemisinin resistance. The data completeness of key variables (species, country of acquisition, and resident status) was lower in 2017 (74.4%) than in 2016 (79.4%).
Interpretation
The number of reported malaria cases in 2017 continued a decades-long increasing trend, and for the second year in a row the highest number of cases since 1971 have been reported. Despite progress in malaria control in recent years, the disease remains endemic in many areas globally. The importation of malaria reflects the overall increase in global travel to and from these areas. Fifty-six percent of all cases were among persons who had traveled from West Africa, and among U.S. civilians, visiting friends and relatives was the most common reason for travel (73.1%). Frequent international travel combined with the inadequate use of Prevention measures by travelers resulted in the highest number of imported malaria cases detected in the U.S. in 4 decades.
Public Health Actions
The best way to prevent malaria is to take chemoprophylaxis medication during travel to a country where malaria is endemic. Adherence to recommended malaria Prevention strategies among U.S. travelers would reduce the numbers of imported cases; reasons for nonadherence include prematurely stopping after leaving the area where malaria was endemic, forgetting to take the medication, and experiencing a side effect. Travelers might not understand the risk that malaria poses to them; thus, health care providers should incorporate risk education to motivate travelers to be adherent to chemoprophylaxis. Malaria infections can be fatal if not diagnosed and treated promptly with antimalarial medications appropriate for the patient’s age, medical History, the likely country of malaria acquisition, and previous use of antimalarial chemoprophylaxis. Antimalarial use for chemoprophylaxis and treatment should be informed by the most recent guidelines, which are frequently updated. In 2018, two formulations of tafenoquine (i.e., Arakoda and Krintafel) were approved by the Food and Drug Administration (FDA) for use in the U.S. Arakoda was approved for use by adults for chemoprophylaxis; the regimen requires a predeparture loading dose, taking the medication weekly during travel, and a short course post travel. The Arakoda chemoprophylaxis regimen is shorter than alternative regimens, which could possibly improve adherence. This medication also might prevent relapses. Krintafel was approved for radical cure of P. vivax infections in those aged >16 years and should be co-administered with chloroquine (https://www.cdc.gov/malaria/new_info/2020/tafenoquine_2020.html). In April 2019, intravenous artesunate became the first-line medication for treatment of severe malaria in the U.S. Artesunate was recently FDA approved but is not yet commercially available. The drug can be obtained from CDC under an investigational new drug protocol. Detailed Rec. for preventing malaria are available to the general public at the CDC website (https://www.cdc.gov/malaria/travelers/drugs.html). Health care providers should consult the CDC Guidelines for Treatment of Malaria in the U.S. and contact the CDC’s Malaria Hotline for case management advice when needed. Malaria treatment Rec. are available online (https://www.cdc.gov/malaria/Diagnosis_treatment) and from the Malaria Hotline (770-488-7788 or toll-free 855-856-4713). Persons submitting malaria case reports (care providers, laboratories, and state and local public health officials) should provide complete information because incomplete reporting compromises case investigations and efforts to prevent infections and examine Trends in malaria cases. Molecular Surveillance of antimalarial drug resistance markers (https://www.cdc.gov/malaria/features/ars.html) enables CDC to track, guide treatment, and manage drug resistance in malaria parasites both domestically and internationally. More samples are needed to improve the completeness of antimalarial drug resistance analysis; therefore, CDC requests that blood specimens be submitted for any case of malaria diagnosed in the U.S.
-
Subjects:
-
Source:Morbidity and Mortality Weekly Report (MMWR): Surveillance Summaries, 2021; v. 70, no. 2
-
Series:
-
DOI:
-
ISSN:1546-0738 (print) ; 1545-8636 (digital)
-
Pubmed ID:33735166
-
Pubmed Central ID:PMC8017932
-
Document Type:
-
Name as Subject:
-
Place as Subject:
-
Pages in Document:40 pdf pages
-
Volume:70
-
Issue:2
-
Collection(s):
-
Main Document Checksum:urn:sha-512:edcfab9081c1f66d629ac4898967ec70d562d55cd31c72e3767d2d4a48fd006770f44926dc7fe92169238bf83077c4e5becdb7aa7e5a15d18b080b0aaf91271f
-
Download URL:
-
File Type:
 [PDF
- 617.32 KB
]
[PDF
- 617.32 KB
]
Supporting Files

File Language:
English

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CDC STACKS serves as an archival repository of CDC-published products including
scientific findings,
journal articles, guidelines, recommendations, or other public health information authored or
co-authored by CDC or funded partners.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
As a repository, CDC STACKS retains documents in their original published format to ensure public access to scientific information.
You May Also Like
COLLECTION
Morbidity and Mortality Weekly Report (MMWR)