
i
The Validity of Discharge Billing Codes Reflecting Severe Maternal Morbidity
-
2016 September
Source: Anesth Analg. 123(3):731-738
 [PDF-441.81 KB]
[PDF-441.81 KB]
Details:
-
Alternative Title:Anesth Analg
-
Personal Author:
-
Description:BACKGROUND
Discharge diagnoses are used to track national trends and patterns of maternal morbidity. There are few data regarding the validity of the International Classification of Diseases (ICD) codes used for this purpose. The goal of our study was to try to better understand the validity of administrative data being used to monitor and assess trends in morbidity.
METHODS
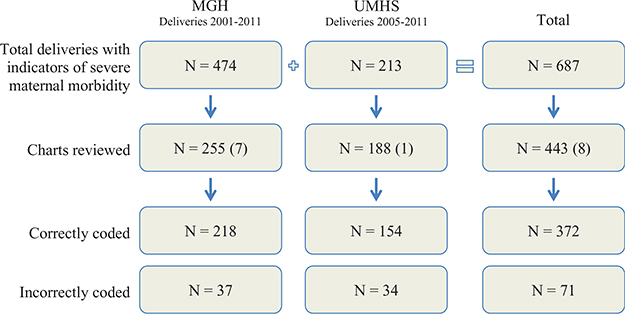
Hospital stay billing records were queried to identify all delivery admissions at the Massachusetts General Hospital for the time period 2001 to 2011 and the University of Michigan Health System for the time period 2005 to 2011. From this, we identified patients with ICD-9-Clinical Modification (CM) diagnosis and procedure codes indicative of severe maternal morbidity. Each patient was classified with 1 of 18 different medical/obstetric categories (conditions or procedures) based on the ICD-9-CM code that was recorded. Within each category, 20 patients from each institution were selected at random, and the corresponding medical charts were reviewed to determine whether the ICD-9-CM code was assigned correctly. The percentage of correct codes for each of 18 preselected clinical categories was calculated yielding a positive predictive value (PPV) and 99% confidence interval (CI).
RESULTS
The overall number of correctly assigned ICD-9-CM codes, or PPV, was 218 of 255 (86%; CI, 79%–90%) and 154 of 188 (82%; CI, 74%–88%) at Massachusetts General Hospital and University of Michigan Health System, respectively (combined PPV, 372/443 [84%; CI, 79–88%]). Codes within 4 categories (Hysterectomy, Pulmonary edema, Disorders of fluid, electrolyte and acid–base balance, and Sepsis) had a 99% lower confidence limit ≥75%. Codes within 8 additional categories demonstrated a 99% lower confidence limit between 74% and 50% (Acute respiratory distress, Ventilation, Other complications of obstetric surgery, Disorders of coagulation, Cardiomonitoring, Acute renal failure, Thromboembolism, and Shock). Codes within 6 clinical categories demonstrated a 99% lower confidence limit <50% (Puerperal cerebrovascular disorders, Conversion of cardiac rhythm, Acute heart failure [includes arrest and fibrillation], Eclampsia, Neurotrauma, and Severe anesthesia complications).
CONCLUSIONS
ICD-9-CM codes capturing severe maternal morbidity during delivery hospitalization demonstrate a range of PPVs. The PPV was high when objective supportive evidence, such as laboratory values or procedure documentation supported the ICD-9-CM code. The PPV was low when greater judgment, interpretation, and synthesis of the clinical data (signs and symptoms) was required to support a code, such as with the category Severe anesthesia complications. As a result, these codes should be used for administrative research with more caution compared with codes primarily defined by objective data.
-
Subjects:
-
Source:
-
Pubmed ID:27387839
-
Pubmed Central ID:PMC7481827
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files




More +
You May Also Like

Sears, Jeanne M.
 ;
;
Rundell, Sean D.
[PDF - 783.99 KB]
 [PDF - 502.39 KB]
[PDF - 502.39 KB]
 Email
CDC-INFO
Email
CDC-INFO









