
i
Universal versus conditional day 3 follow-up for children with non-severe unclassified fever at the community level in the Democratic Republic of the Congo: A cluster-randomized, community-based non-inferiority trial
-
Apr 17 2018
Source: PLoS Med. 15(4). -
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
The World Health Organization’s integrated community case management (iCCM) guidelines recommend that all children presenting with uncomplicated fever and no danger signs return for follow-up on day 3 following the initial consultation on day 1. Such fevers often resolve rapidly, however, and previous studies suggest that expectant home care for uncomplicated fever can be safely recommended. We aimed to determine if a conditional follow-up visit was non-inferior to a universal follow-up visit for these children.
Methods and findings
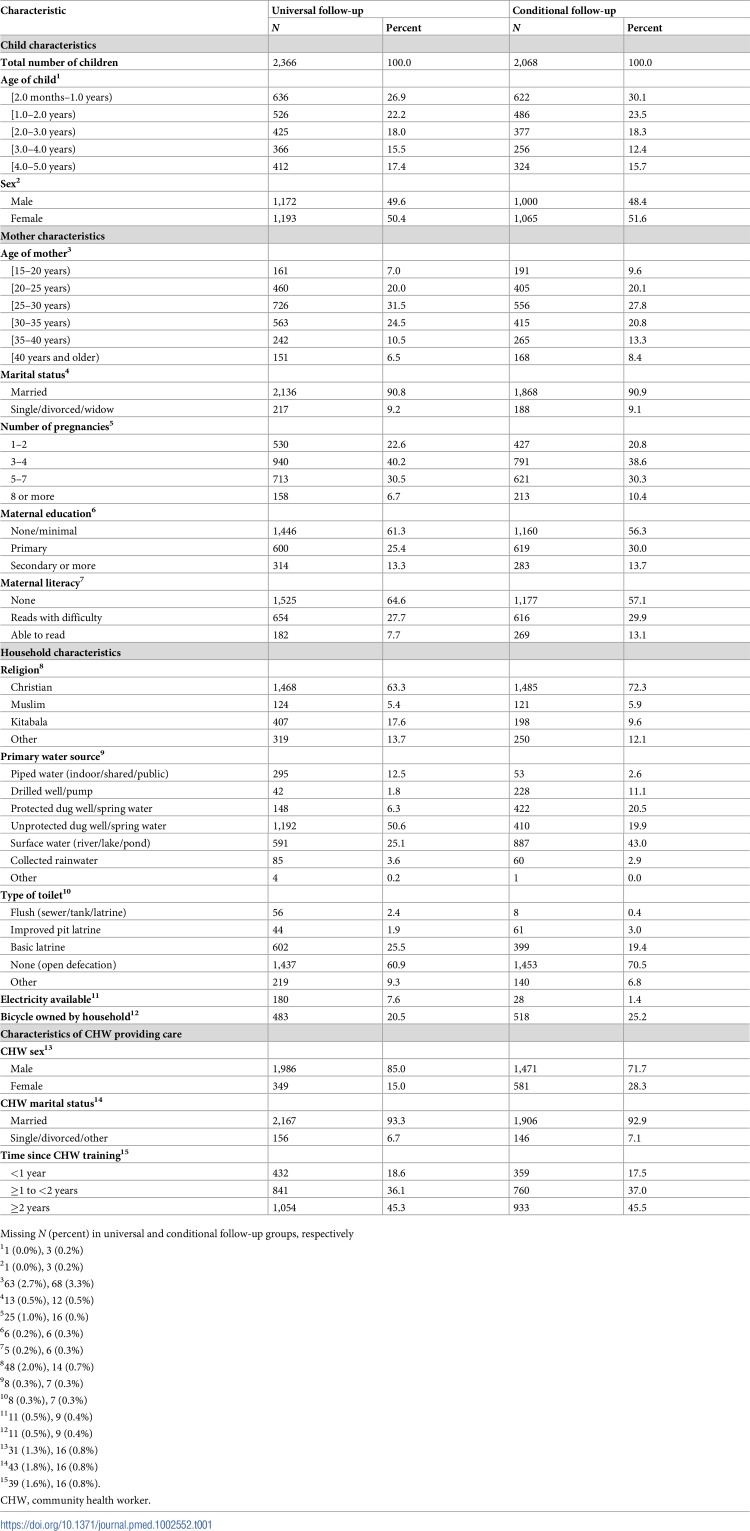
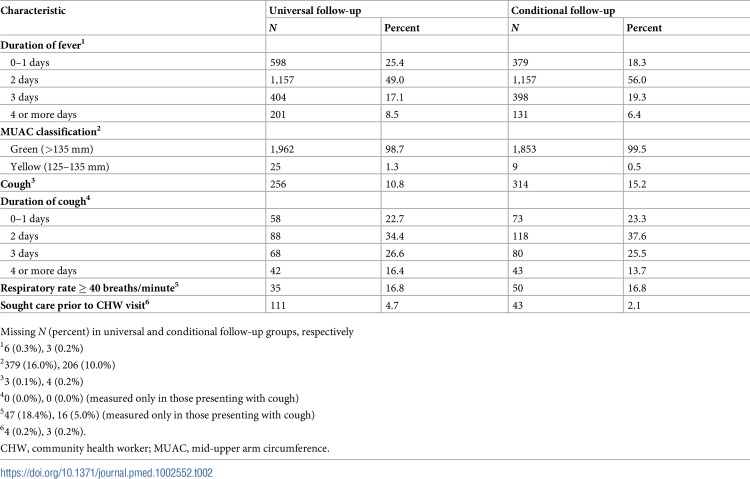
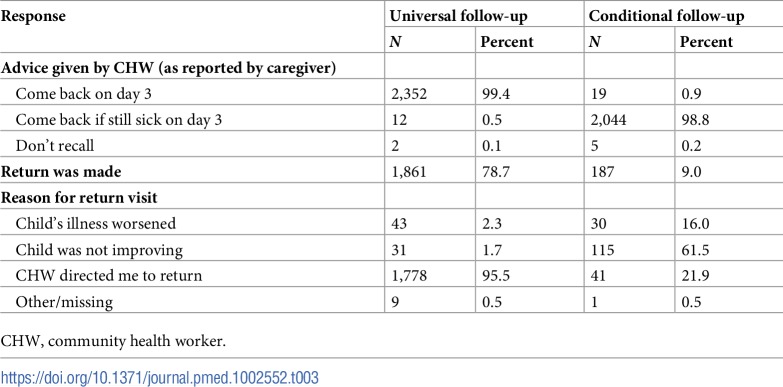
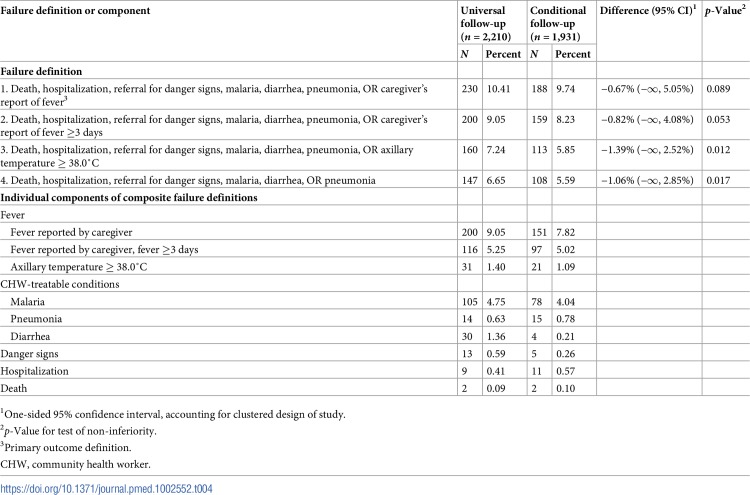
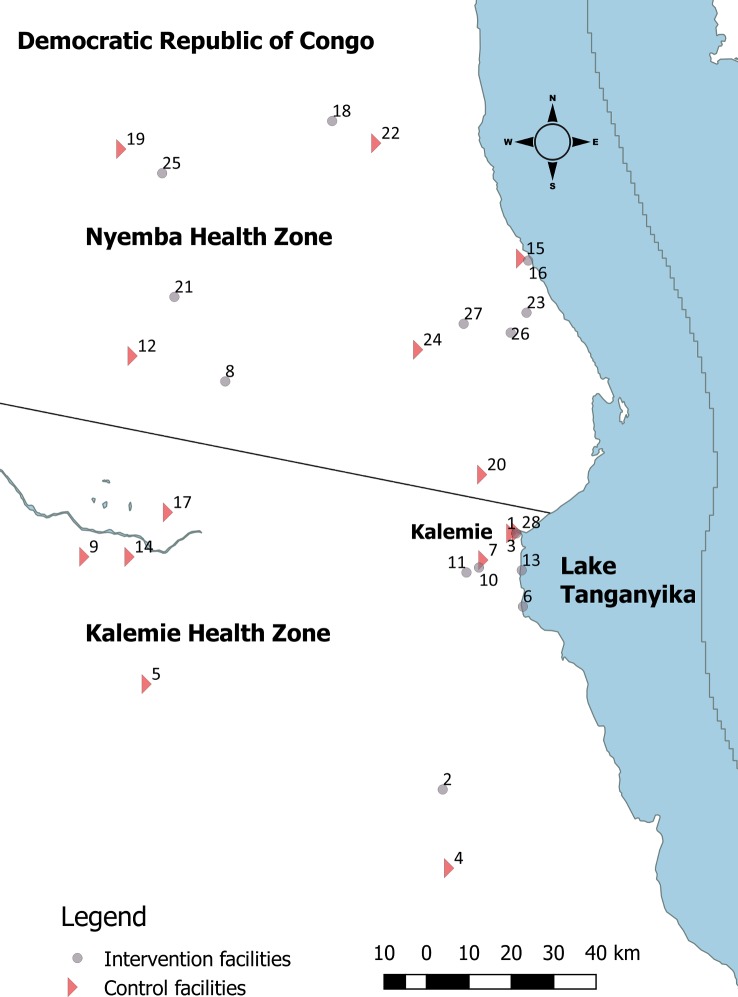
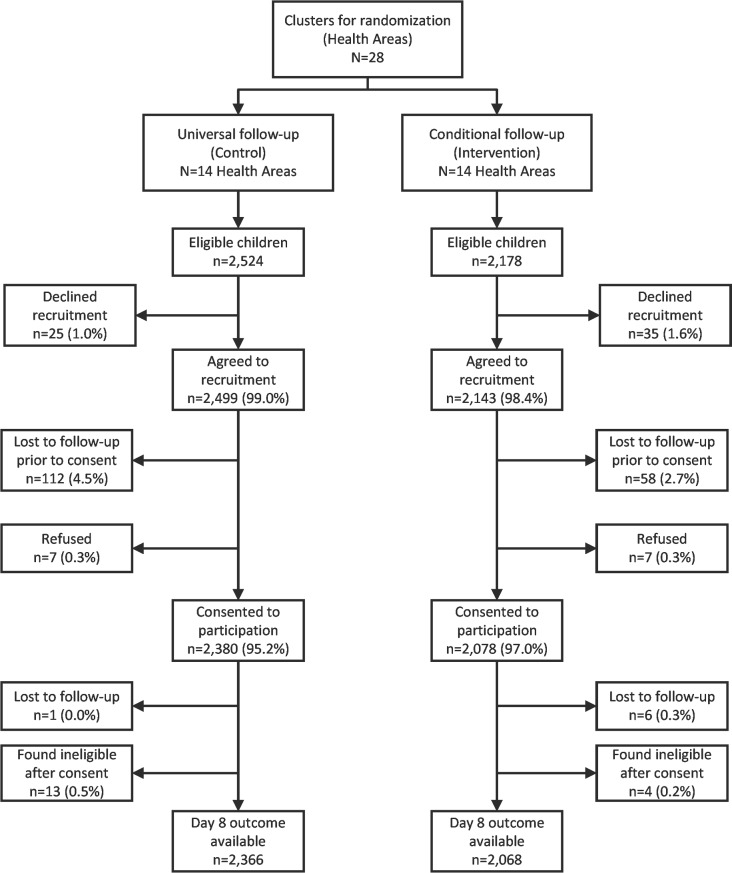
We conducted a cluster-randomized, community-based non-inferiority trial among children 2–59 months old presenting to community health workers (CHWs) with non-severe unclassified fever in Tanganyika Province, Democratic Republic of the Congo. Clusters (n = 28) of CHWs were randomized to advise caregivers to either (1) return for a follow-up visit on day 3 following the initial consultation on day 1, regardless of illness resolution (as per current WHO guidelines; universal follow-up group) or (2) return for a follow-up visit on day 3 only if illness continued (conditional follow-up group). Children in both arms were assessed again at day 8, and classified as a clinical failure if fever (caregiver-reported), malaria, diarrhea, pneumonia, or decline of health status (development of danger signs, hospitalization, or death) was noted (failure definition 1). Alternative failure definitions were examined, whereby caregiver-reported fever was first restricted to caregiver-reported fever of at least 3 days (failure definition 2) and then replaced with fever measured via axillary temperature (failure definition 3). Study participants, providers, and investigators were not masked. Among 4,434 enrolled children, 4,141 (93.4%) met the per-protocol definition of receipt of the arm-specific advice from the CHW and a timely day 8 assessment (universal follow-up group: 2,210; conditional follow-up group: 1,931). Failure was similar (difference: –0.7%) in the conditional follow-up group (n = 188, 9.7%) compared to the universal follow-up group (n = 230, 10.4%); however, the upper bound of a 1-sided 95% confidence interval around this difference (−∞, 5.1%) exceeded the prespecified non-inferiority margin of 4.0% (non-inferiority p = 0.089). When caregiver-reported fever was restricted to fevers lasting ≥3 days, failure in the conditional follow-up group (n = 159, 8.2%) was similar to that in the universal follow-up group (n = 200, 9.1%) (difference: −0.8%; 95% CI: −∞, 4.1%; p = 0.053). If caregiver-reported fever was replaced by axillary temperature measurement in the definition of failure, failure in the conditional follow-up group (n = 113, 5.9%) was non-inferior to that in the universal follow-up group (n = 160, 7.2%) (difference: −1.4%; 95% CI: −∞, 2.5%; p = 0.012). In post hoc analysis, when the definition of failure was limited to malaria, diarrhea, pneumonia, development of danger signs, hospitalization, or death, failure in the conditional follow-up group (n = 108, 5.6%) was similar to that in the universal follow-up group (n = 147, 6.7%), and within the non-inferiority margin (95% CI: −∞, 2.9%; p = 0.017). Limitations include initial underestimation of the proportion of clinical failures as well as substantial variance in cluster-specific failure rates, reducing the precision of our estimates. In addition, heightened security concerns slowed recruitment in the final months of the study.
Conclusions
We found that advising caregivers to return only if children worsened or remained ill on day 3 resulted in similar rates of caregiver-reported fever and other clinical outcomes on day 8, compared to advising all caregivers to return on day 3. Policy-makers could consider revising guidelines for management of uncomplicated fever within the iCCM framework.
Trial registration
ClinicalTrials.gov NCT02595827
Why was this study done?
What did the researchers do and find?
What do these findings mean?
-
Subjects:
-
Source:
-
Pubmed ID:29664951
-
Pubmed Central ID:PMC5903590
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-

pdf 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
xml 
pdf 
docx 
docx
 [PDF-1.33 MB]
[PDF-1.33 MB]
Details:
Supporting Files



More +


 Email
CDC-INFO
Email
CDC-INFO









