
i
Resisting and tolerating P. falciparum in pregnancy under different malaria transmission intensities
-
Jul 17 2017
Source: BMC Med. 15. -
Alternative Title:BMC Med
-
Personal Author:
-
Description:Background
Resistance and tolerance to Plasmodium falciparum can determine the progression of malaria disease. However, quantitative evidence of tolerance is still limited. We investigated variations in the adverse impact of P. falciparum infections among African pregnant women under different intensities of malaria transmission.
Methods
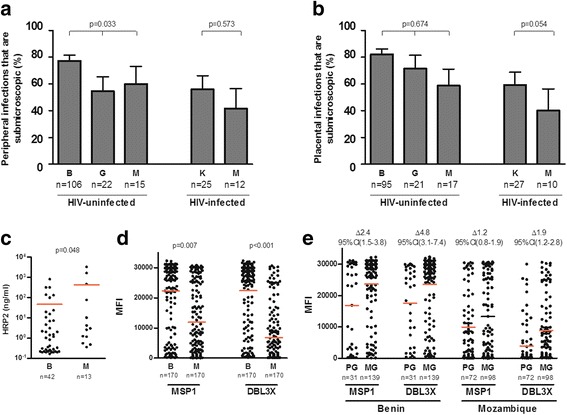
P. falciparum at delivery was assessed by microscopy, quantitative PCR (qPCR) and placental histology in 946 HIV-uninfected and 768 HIV-infected pregnant women from Benin, Gabon, Kenya and Mozambique. Resistance was defined by the proportion of submicroscopic infections and the levels of anti-parasite antibodies quantified by Luminex, and tolerance by the relationship of pregnancy outcomes with parasite densities at delivery.
Results
P. falciparum prevalence by qPCR in peripheral and/or placental blood of HIV-uninfected Mozambican, Gabonese and Beninese women at delivery was 6% (21/340), 11% (28/257) and 41% (143/349), respectively. The proportion of peripheral submicroscopic infections was higher in Benin (83%) than in Mozambique (60%) and Gabon (55%; P = 0.033). Past or chronic placental P. falciparum infection was associated with an increased risk of preterm birth in Mozambican newborns (OR = 7.05, 95% CI 1.79 to 27.82). Microscopic infections were associated with reductions in haemoglobin levels at delivery among Mozambican women (–1.17 g/dL, 95% CI –2.09 to –0.24) as well as with larger drops in haemoglobin levels from recruitment to delivery in Mozambican (–1.66 g/dL, 95% CI –2.68 to –0.64) and Gabonese (–0.91 g/dL, 95% CI –1.79 to –0.02) women. Doubling qPCR-peripheral parasite densities in Mozambican women were associated with decreases in haemoglobin levels at delivery (–0.16 g/dL, 95% CI –0.29 to –0.02) and increases in the drop of haemoglobin levels (–0.29 g/dL, 95% CI –0.44 to –0.14). Beninese women had higher anti-parasite IgGs than Mozambican women (P < 0.001). No difference was found in the proportion of submicroscopic infections nor in the adverse impact of P. falciparum infections in HIV-infected women from Kenya (P. falciparum prevalence by qPCR: 9%, 32/351) and Mozambique (4%, 15/417).
Conclusions
The lowest levels of resistance and tolerance in pregnant women from areas of low malaria transmission were accompanied by the largest adverse impact of P. falciparum infections. Exposure-dependent mechanisms developed by pregnant women to resist the infection and minimise pathology can reduce malaria-related adverse outcomes. Distinguishing both types of defences is important to understand how reductions in transmission can affect malaria disease.
Trial registration
ClinicalTrials.gov NCT00811421. Registered 18 December 2008.
Electronic supplementary material
The online version of this article (doi:10.1186/s12916-017-0893-6) contains supplementary material, which is available to authorized users.
-
Subjects:
-
Source:
-
Pubmed ID:28712360
-
Pubmed Central ID:PMC5513247
-
Document Type:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-
jpeg
docx
bin
gif
jpeg
gif
jpeg
gif
jpeg
gif
 [PDF-925.51 KB]
[PDF-925.51 KB]
Details:
Supporting Files






More +
You May Also Like
 [PDF - 309.84 KB]
[PDF - 309.84 KB]

 Email
CDC-INFO
Email
CDC-INFO









