
i
Evaluation of a laboratory quality assurance pilot programme for malaria diagnostics in low-transmission areas of Kenya, 2013
-
May 25 2017
Source: Malar J. 16. -
Alternative Title:Malar J
-
Personal Author:
-
Description:Background
One objective of the Kenya National Malaria Strategy 2009–2017 is scaling access to prompt diagnosis and effective treatment. In 2013, a quality assurance (QA) pilot was implemented to improve accuracy of malaria diagnostics at selected health facilities in low-transmission counties of Kenya. Trends in malaria diagnostic and QA indicator performance during the pilot are described.
Methods
From June to December 2013, 28 QA officers provided on-the-job training and mentoring for malaria microscopy, malaria rapid diagnostic tests and laboratory QA/quality control (QC) practices over four 1-day visits at 83 health facilities. QA officers observed and recorded laboratory conditions and practices and cross-checked blood slides for malaria parasite presence, and a portion of cross-checked slides were confirmed by reference laboratories.
Results
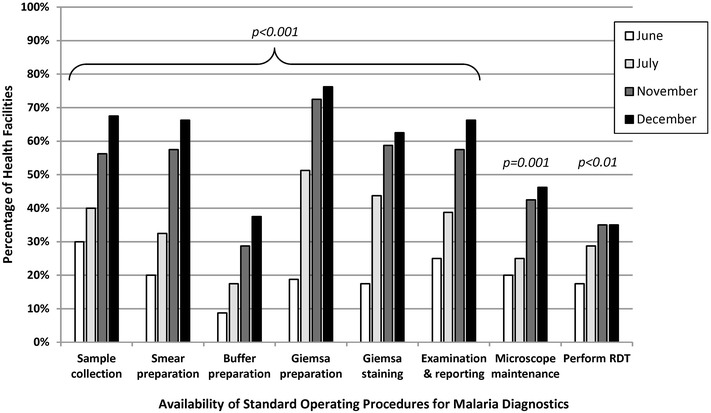
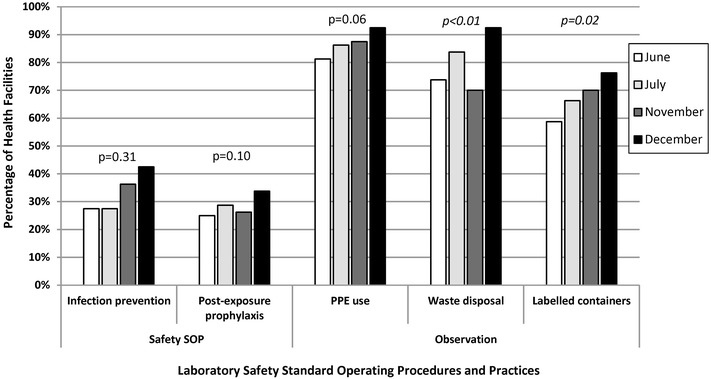
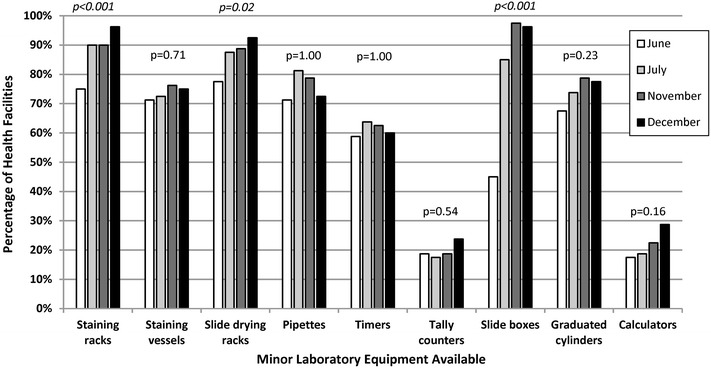
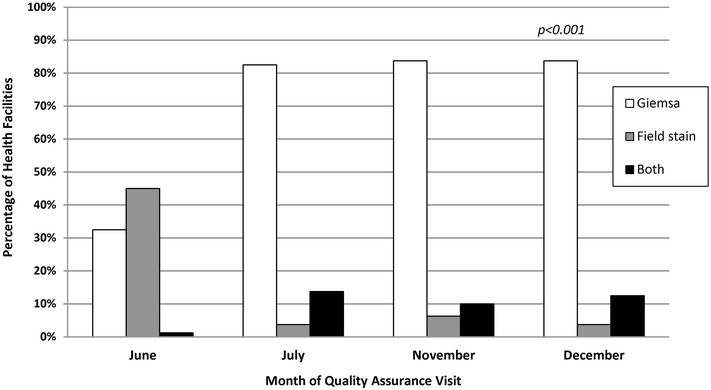
Eighty (96%) facilities completed the pilot. Among 315 personnel at pilot initiation, 13% (n = 40) reported malaria diagnostics training within the previous 12 months. Slide positivity ranged from 3 to 7%. Compared to the reference laboratory, microscopy sensitivity ranged from 53 to 96% and positive predictive value from 39 to 53% for facility staff and from 60 to 96% and 52 to 80%, respectively, for QA officers. Compared to reference, specificity ranged from 88 to 98% and negative predictive value from 98 to 99% for health-facility personnel and from 93 to 99% and 99%, respectively, for QA officers. The kappa value ranged from 0.48–0.66 for facility staff and 0.57–0.84 for QA officers compared to reference. The only significant test performance improvement observed for facility staff was for specificity from 88% (95% CI 85–90%) to 98% (95% CI 97–99%). QA/QC practices, including use of positive-control slides, internal and external slide cross-checking and recording of QA/QC activities, all increased significantly across the pilot (p < 0.001). Reference material availability also increased significantly; availability of six microscopy job aids and seven microscopy standard operating procedures increased by a mean of 32 percentage points (p < 0.001) and 38 percentage points (p < 0.001), respectively.
Conclusions
Significant gains were observed in malaria QA/QC practices over the pilot. However, these advances did not translate into improved accuracy of malaria diagnostic performance perhaps because of the limited duration of the QA pilot implementation.
Electronic supplementary material
The online version of this article (doi:10.1186/s12936-017-1856-2) contains supplementary material, which is available to authorized users.
-
Subjects:
-
Source:
-
Pubmed ID:28545579
-
Pubmed Central ID:PMC5445328
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-
jpeg
gif
jpeg
gif
jpeg
pdf
bin
gif
jpeg
gif
jpeg
gif
jpeg
gif
 [PDF-1.23 MB]
[PDF-1.23 MB]
Details:
Supporting Files



More +


 Email
CDC-INFO
Email
CDC-INFO









