
i
Structural Level Differences in the Mother-to-Child HIV Transmission Rate in South Africa: A Multilevel Assessment of Individual-, Health Facility-, and Provincial-Level Predictors of Infant HIV Transmission
-
Apr 15 2017
Source: J Acquir Immune Defic Syndr. 2017; 74(5):523-530.
 [PDF-293.70 KB]
[PDF-293.70 KB]
Details:
-
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:
-
Description:Objectives:
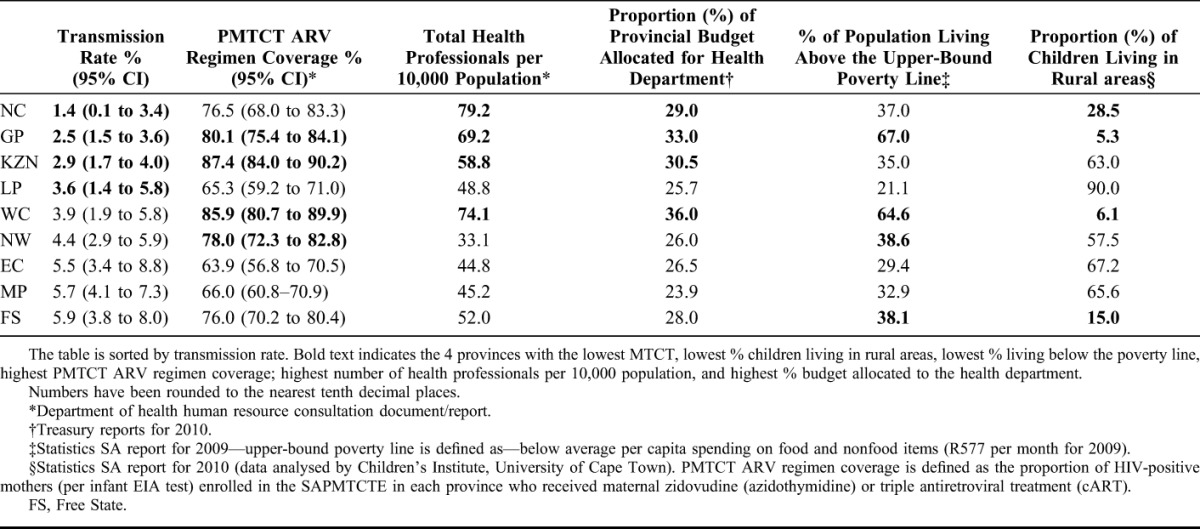
In 2010, South Africa reported an early mother-to-child transmission (MTCT) rate of 3.5% at 4–8 weeks postpartum. Provincial early MTCT rates ranged from 1.4% [95% confidence interval (CI): 0.1 to 3.4] to 5.9% (95% CI: 3.8 to 8.0). We sought to determine reasons for these geographic differences in MTCT rates.
Methods:
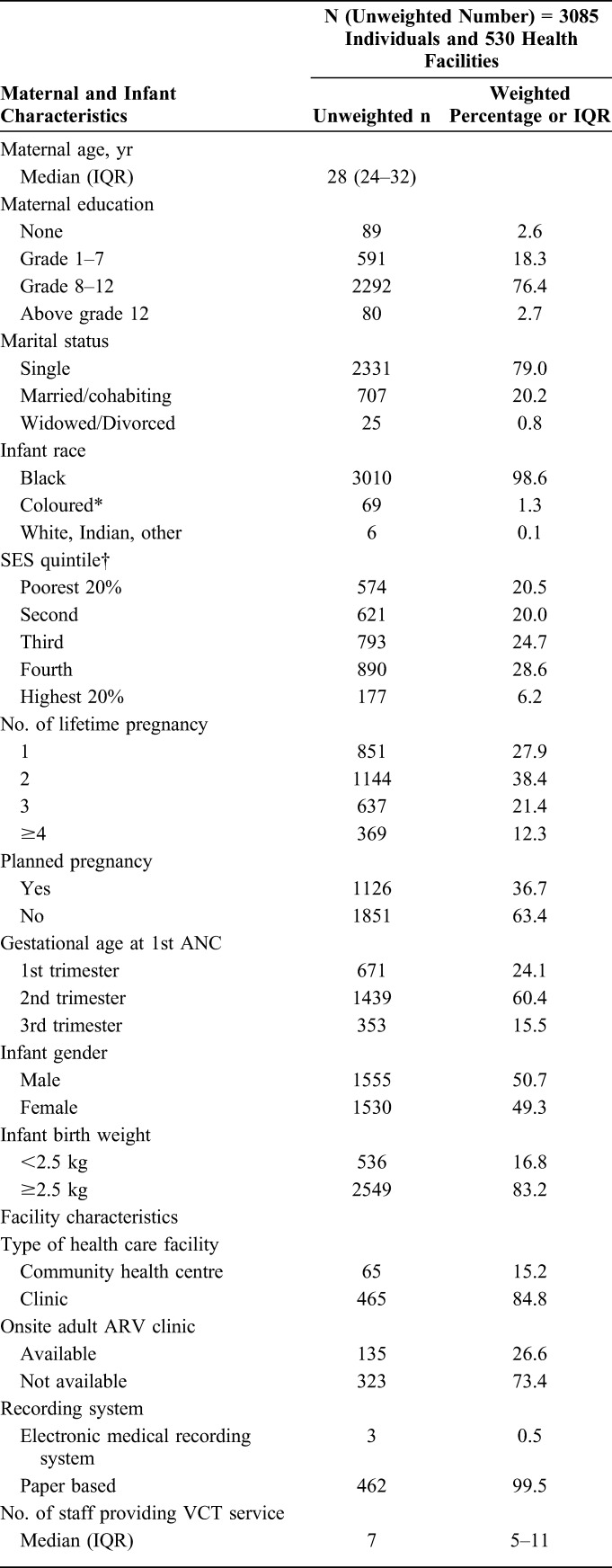
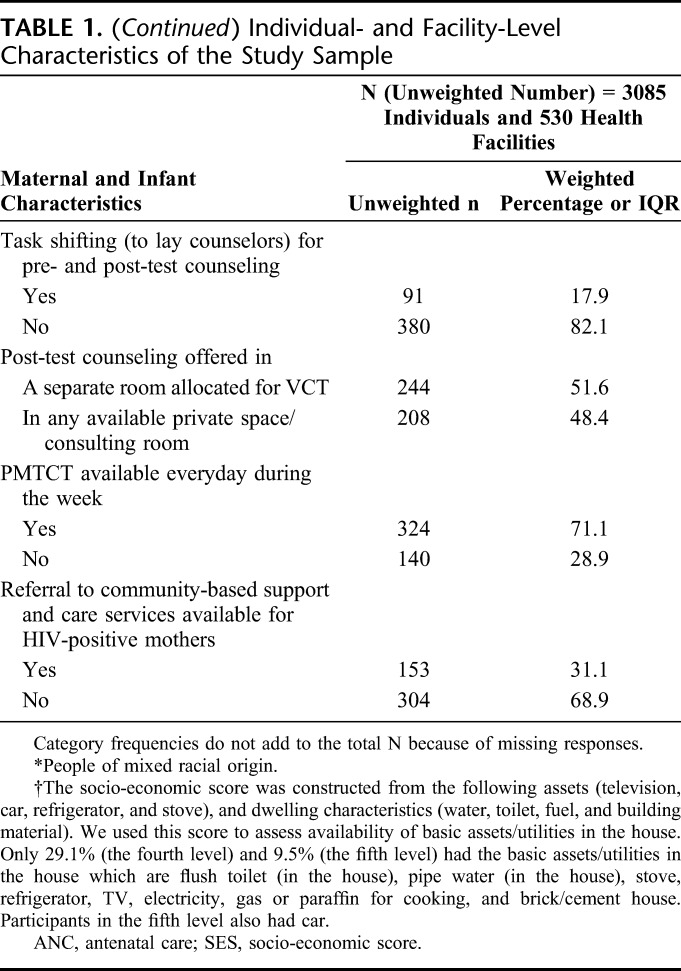
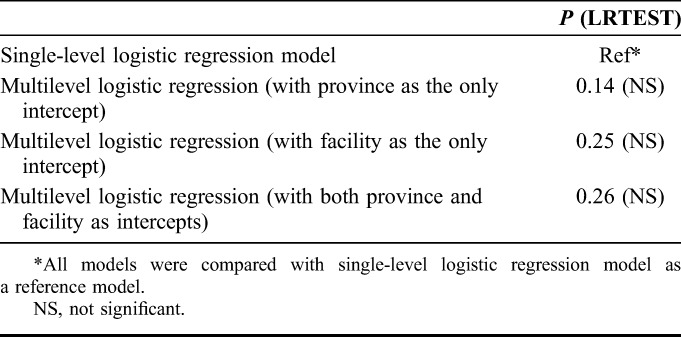
This study used multilevel modeling using 2010 South African prevention of mother-to-child transmission (PMTCT) evaluation (SAPMTCTE) data from 530 facilities. Interview data and blood samples of infants were collected from 3085 mother–infant pairs at 4–8 weeks postpartum. Facility-level data on human resources, referral systems, linkages to care, and record keeping were collected through facility staff interviews. Provincial level data were gathered from publicly available data (eg, health professionals per 10,000 population) or aggregated at province-level from the SAPMTCTE (PMTCT maternal-infant antiretroviral (ARV) coverage). Variance partition coefficients and odds ratios (for provincial facility- and individual-level factors influencing MTCT) from multilevel modeling are reported.
Results:
The provincial- (5.0%) and facility-level (1.4%) variance partition coefficients showed no substantive geographic variation in early MTCT. In multivariable analysis accounting for the multilevel nature of the data, the following were associated with early MTCT: individual-level—low maternal–infant ARV uptake [adjusted odds ratio (AOR) = 2.5, 95% CI: 1.7 to 3.5], mixed breastfeeding (AOR = 1.9, 95% CI: 1.3 to 2.9) and maternal age <20 years (AOR 1.8, 95% CI: 1.1 to 3.0); facility-level–insufficient (≤2) health care-personnel for HIV-testing services (AOR = 1.8, 95% CI: 1.1 to 3.0); provincial-level PMTCT ARV (maternal–infant) coverage lower than 80% (AOR = 1.4, 95% CI: 1.1 to 1.9), and number of health professionals per 10,000 population (AOR = 0.99, 95% CI: 0.98 to 0.99).
Conclusions:
There was no substantial province-/facility-level MTCT difference. This could be due to good overall performance in reducing early MTCT. Disparities in human resource allocation (including allocation of insufficient health care personnel for testing and care at facility level) and PMTCT coverage influenced overall PMTCT programme performance. These are long-standing systemic problems that impact quality of care.
-
Subjects:
-
Pubmed ID:28107227
-
Pubmed Central ID:PMC5351751
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files
-

gif 
jpeg 
gif 
jpeg 
bin 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg





More +


 Email
CDC-INFO
Email
CDC-INFO









