
i
Beyond Body Mass Index: Advantages of Abdominal Measurements for Recognizing Cardiometabolic Disorders
-
Aug 21 2015
Source: Am J Med. 129(1):74-81.e2. -
Alternative Title:Am J Med
-
Personal Author:
-
Description:BACKGROUND
The clinical recognition of cardiometabolic disorders might be enhanced by anthropometry based on the sagittal abdominal diameter (SAD; also called “abdominal height”) or waist circumference rather than on weight. Direct comparisons of body mass index (BMI, weight/height2) with SAD/height ratio (SADHtR) or waist circumference/height ratio (WHtR) have not previously been tested in nationally representative populations.
METHODS
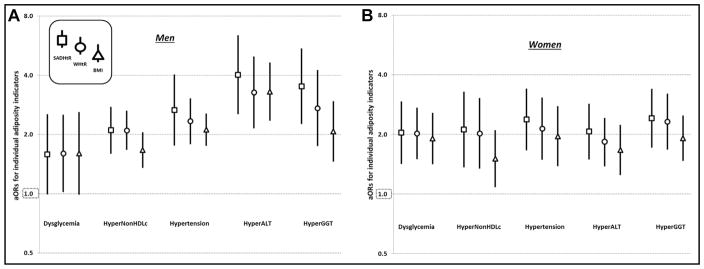
Nonpregnant adults without diagnosed diabetes (ages 20–64 years; n = 3071) provided conventional anthropometry and supine SAD (by sliding-beam caliper) in the 2011–2012 US National Health and Nutrition Examination Survey. Population-weighted, logistic models estimated how strongly each anthropometric indicator was associated with 5 cardiometabolic disorders: Dysglycemia (glycated hemoglobin ≥5.7%), HyperNonHDLc (non-high-density-lipoprotein [HDL] cholesterol ≥4.14 mmol/L, or taking anticholesteremic medications), Hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, or taking antihypertensive medications), HyperALT (alanine transaminase ≥p75 [75th percentile, sex-specific]), and HyperGGT (gamma-glutamyltransferase ≥p75 [sex-specific]).
RESULTS
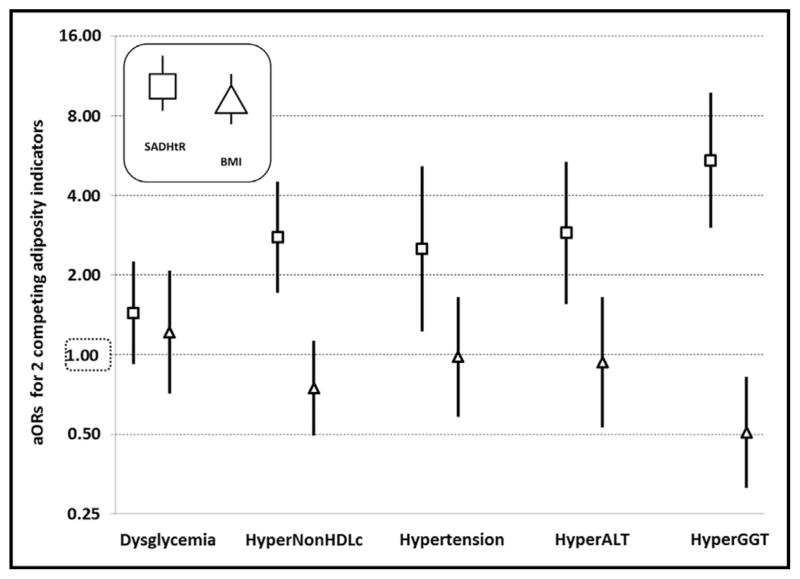
After scaling each indicator, adjusted odds ratios (aORs) tended to be highest for SADHtR and lowest for BMI when identifying each disorder except dysglycemia. When SADHtR entered models simultaneously with BMI, the aORs for BMI no longer directly identified any condition, whereas SADHtR identified persons with HyperNonHDLc by aOR 2.78 (95% confidence interval [CI], 1.71–4.51), Hypertension by aOR 2.51 (95% CI, 1.22–5.15), HyperALT by aOR 2.89 (95% CI, 1.56–5.37), and HyperGGT by aOR 5.43 (95% CI, 3.01–9.79). WHtR competed successfully against BMI with regard to Dysglycemia, Hyper-NonHDLc, and HyperGGT. c-Statistics of SADHtR and WHtR were higher than those of BMI (P <.001) for identifying HyperNonHDLc and HyperGGT.
CONCLUSIONS
Among nonelderly adults, SADHtR or WHtR recognized cardiometabolic disorders better than did the BMI.
-
Subjects:
-
Source:
-
Pubmed ID:26302146
-
Pubmed Central ID:PMC5292922
-
Document Type:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-

pdf 
bin 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg
 [PDF-673.64 KB]
[PDF-673.64 KB]
Details:
Supporting Files


More +
You May Also Like
 [PDF - 287.98 KB]
[PDF - 287.98 KB]
 [PDF - 339.71 KB]
[PDF - 339.71 KB]
 Email
CDC-INFO
Email
CDC-INFO









