
i
Effect of Pregnancy on Response to Antiretroviral Therapy in HIV-Infected African Women
-
Jan 01 2017
Source: J Acquir Immune Defic Syndr. 2016; 74(1):38-43. -
Alternative Title:J Acquir Immune Defic Syndr
-
Personal Author:
-
Description:Background:
While most recent evidence does not support a role for pregnancy in accelerating HIV disease progression, very little information is available on the effects of incident pregnancy in response to antiretroviral therapy (ART). Hormonal, immune, and behavioral changes during pregnancy may influence response to ART. We sought to explore the effects of incident pregnancy (after ART initiation) on virologic, immunologic, and clinical response to ART.
Methods:
Data were collected from HIV-infected women participating in 3 prospective studies (Partners in Prevention Herpes simplex virus/HIV Transmission Study, Couples Observational Study, and Partners Preexposure Prophylaxis Study) from 7 countries in Africa from 2004 to 2012. Women were included in this analysis if they were ≤45 years of age, were started on ART during the study and were not pregnant at ART initiation. Pregnancy was treated as a time-dependent exposure variable covering the duration of pregnancy, including all pregnancies occurring after ART initiation. Virologic failure was defined as a viral load (VL) greater than 400 copies per milliliter ≥6 months after ART initiation and viral suppression was defined as VL ≤400 copies per milliliter. Multivariable Cox proportional hazards models were used to assess the association between pregnancy and time to viral suppression, virologic failure, World Health Organization clinical stage III/IV, and death. Linear mixed-effects models were used to assess the association between pregnancy and CD4+ count and VL. All analyses were adjusted for confounders, including pre-ART CD4+ count and plasma VL.
Results:
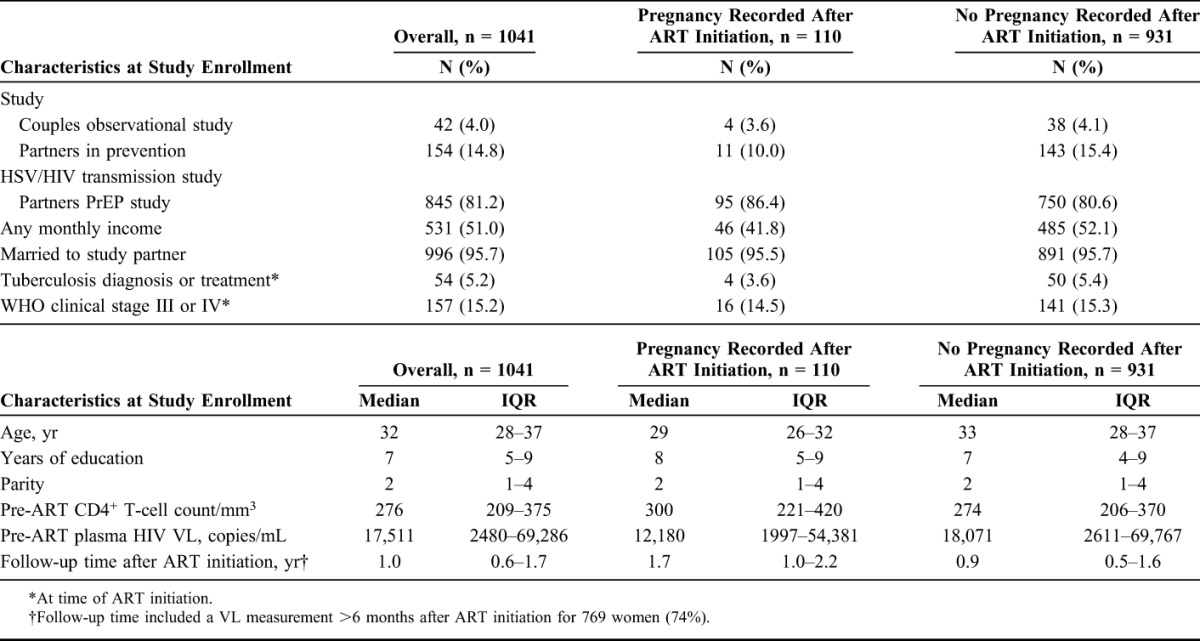
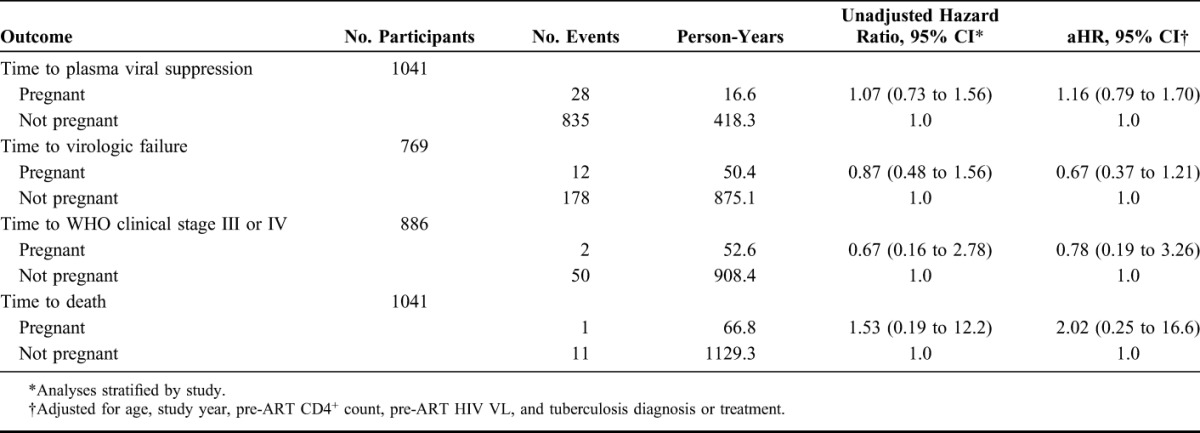
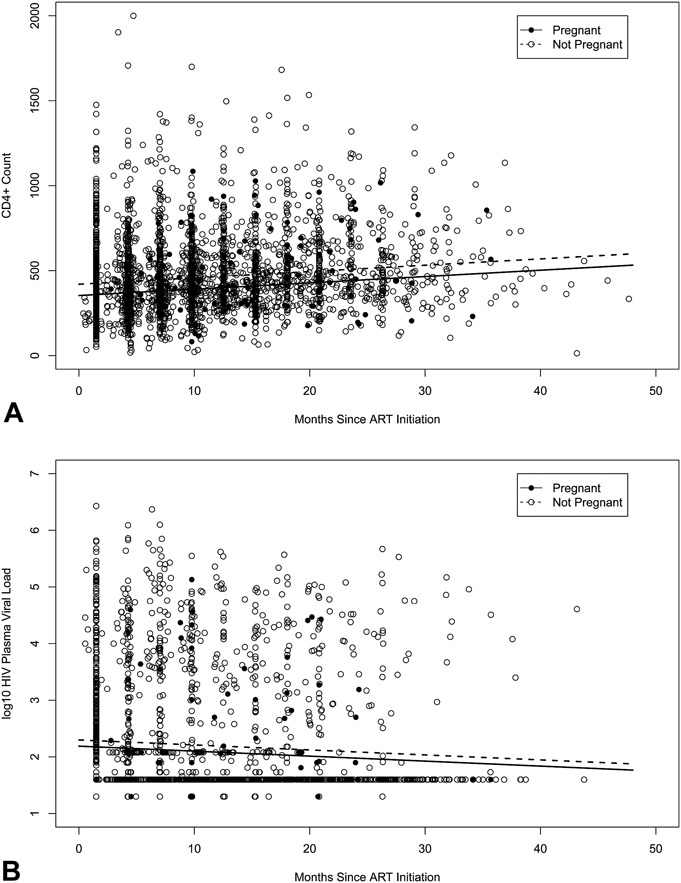
A total of 1041 women were followed, contributing 1196.1 person-years of follow-up. Median CD4+ count before ART initiation was 276 cells per cubic millimeter (interquartile range, 209–375); median pre-ART VL was 17,511 copies per milliliter (interquartile range, 2480–69,286). One hundred ten women became pregnant after ART initiation. Pregnancy was not associated with time to viral suppression (adjusted hazard ratio [aHR], 1.20, 95% confidence interval [CI]: 0.82 to 1.77), time to virologic failure (aHR, 0.67, 95% CI: 0.37 to 1.22), time to World Health Organization clinical stage III or IV (aHR, 0.79, 95% CI: 0.19 to 3.30), or time to death (aHR, 2.04, 95% CI: 0.25 to 16.8). Incident pregnancy was associated with an adjusted mean decrease in CD4+ T-cell count of 47.3 cells per cubic millimeter (P < 0.001), but not with difference in VL (P = 0.06).
Conclusions:
For HIV-infected women on ART, incident pregnancy does not affect virologic control or clinical HIV disease progression. A modest decrease in CD4+ T-cell count could be due to physiologic effects of pregnancy.
-
Subjects:
-
Pubmed ID:27787340
-
Pubmed Central ID:PMC5147030
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-
bin 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg
 [PDF-235.82 KB]
[PDF-235.82 KB]
Details:
Supporting Files



More +


 Email
CDC-INFO
Email
CDC-INFO









