
i
The Effect of Highly Active Antiretroviral Therapy on the Survival of HIV-Infected Children in a Resource-Deprived Setting: A Cohort Study
-
Jun 14 2011
Source: PLoS Med. 2011; 8(6). -
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
The effect of highly active antiretroviral therapy (HAART) on the survival of HIV-infected children has not been well quantified. Because most pediatric HIV occurs in low- and middle-income countries, our objective was to provide a first estimate of this effect among children living in a resource-deprived setting.
Methods and Findings
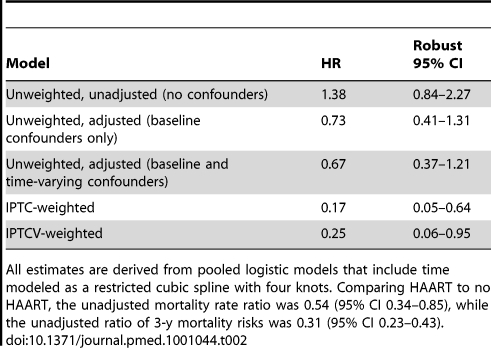
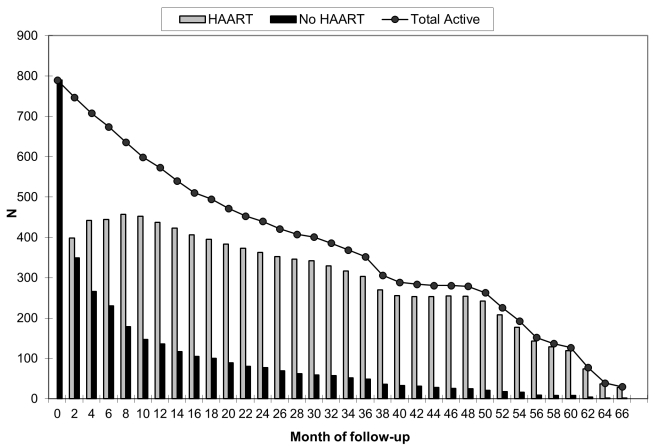
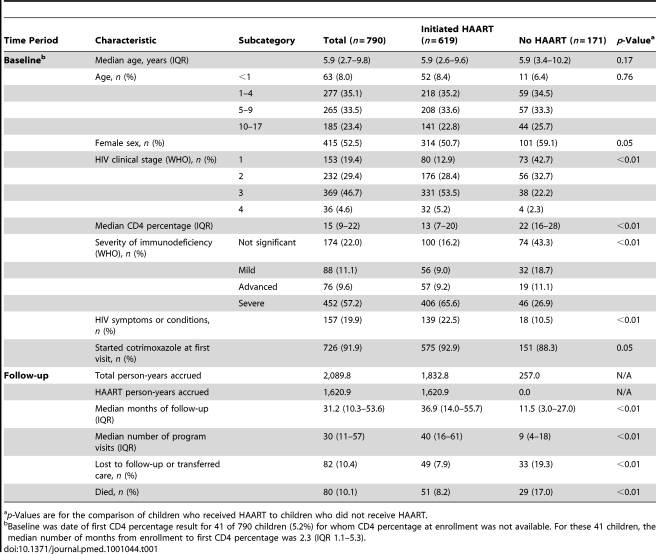
Observational data from HAART-naïve children enrolled into an HIV care and treatment program in Kinshasa, Democratic Republic of the Congo, between December 2004 and May 2010 were analyzed. We used marginal structural models to estimate the effect of HAART on survival while accounting for time-dependent confounders affected by exposure. At the start of follow-up, the median age of the 790 children was 5.9 y, 528 (66.8%) had advanced or severe immunodeficiency, and 405 (51.3%) were in HIV clinical stage 3 or 4. The children were observed for a median of 31.2 mo and contributed a total of 2,089.8 person-years. Eighty children (10.1%) died, 619 (78.4%) initiated HAART, six (0.8%) transferred to a different care provider, and 76 (9.6%) were lost to follow-up. The mortality rate was 3.2 deaths per 100 person-years (95% confidence interval [CI] 2.4–4.2) during receipt of HAART and 6.0 deaths per 100 person-years (95% CI 4.1–8.6) during receipt of primary HIV care only. The mortality hazard ratio comparing HAART with no HAART from a marginal structural model was 0.25 (95% CI 0.06–0.95).
Conclusions
HAART reduced the hazard of mortality in HIV-infected children in Kinshasa by 75%, an estimate that is similar in magnitude but with lower precision than the reported effect of HAART on survival among children in the United States.
Please see later in the article for the Editors' Summary
In 2009, an estimated 2.5 million children were living with HIV, the majority of whom (2.3 million) were in sub-Saharan Africa. Most (90%) of these children acquired HIV from their HIV-infected mothers during pregnancy, birth, or breastfeeding, highlighting the importance of giving effective drugs for the prevention of mother to child transmission. As such interventions are still not widely accessible or available in most resource-limited countries, where the burden of HIV is highest, every day an estimated 1,000 children were newly infected with HIV in 2009, but only 360,000 children were receiving highly active antiretroviral therapy (HAART).
Why Was This Study Done?
Most observational studies of the effects of treatment on child survival have been undertaken in high-income countries, such as Italy and the United States. As most children with HIV live in low-resource areas, where multiple factors, such as delayed presentation to care and a higher incidence of co-occurring conditions, might adversely affect treatment outcomes, there is a specific need for information on the effects of HAART in children with HIV living in low-income countries. Although some investigations have taken place in pediatric cohorts from such countries (for example, Côte d'Ivoire, Haiti, Lesotho, Thailand, and Zambia), the effect of HAART on mortality has not been accurately quantified among children in a resource-deprived setting. Therefore, in this observational clinical cohort study, the researchers investigated the effect of HAART on mortality in HIV-infected children in Kinshasa, in the Democratic Republic of the Congo (DRC).
What Did the Researchers Do and Find?
The researchers analyzed data from 790 children enrolled into an HIV program in Kinshasa, DRC, between December 2004 and May 2010 and used a statistical model (marginal structural models) to adjust for time-dependent confounding factors, such as the fact that HAART is typically initiated in sicker patients, for example, those with lower CD4 cell percentages. Assuming that all children starting HAART received it uninterruptedly throughout follow-up, using this statistical model, the researchers were able to compare the hazard ratio of death had all children initiated HAART to that had no children initiated HAART during follow-up.
What Do These Findings Mean?
These findings show that treatment with HAART markedly improved the survival of children infected with HIV in Kinshasa, DRC, and suggest that HAART is as effective in improving the survival of HIV-infected children in a severely resource-deprived country (still recovering from civil war) as in more resource-privileged settings—an important finding given that the vast majority of children receiving HAART live in resource-poor areas. This study provides additional evidence that accelerating rollout of antiretroviral therapy to children with HIV in resource-poor countries is lifesaving and effective. Future research needs to address how effective HAART is in understudied populations in resource-poor countries, such as undernourished children or those with co-infections such as tuberculosis.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001044.
-
Subjects:
-
Source:
-
Pubmed ID:21695087
-
Pubmed Central ID:PMC3114869
-
Document Type:
-
Funding:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-

jpeg 
gif 
jpeg 
gif 
jpeg 
bin 
gif 
jpeg 
gif
 [PDF-269.47 KB]
[PDF-269.47 KB]
Details:
Supporting Files




More +


 Email
CDC-INFO
Email
CDC-INFO









