
i
A Clinical Trial
-
Mar 29 2011
Source: PLoS Med. 8(3).
 [PDF-394.87 KB]
[PDF-394.87 KB]
Details:
-
Alternative Title:PLoS Med
-
Personal Author:
-
Corporate Authors:
-
Description:Background
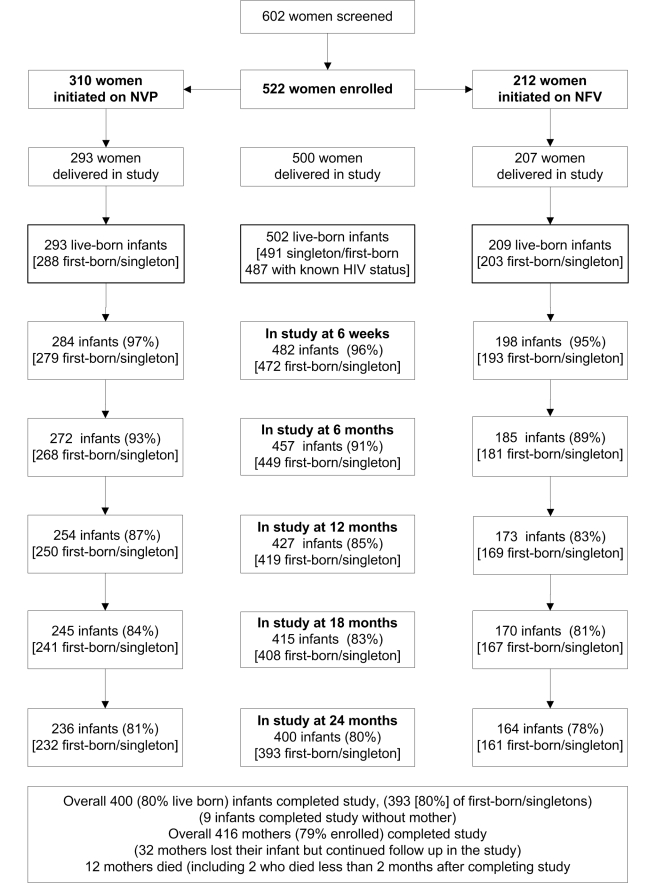
Effective strategies are needed for the prevention of mother-to-child HIV transmission (PMTCT) in resource-limited settings. The Kisumu Breastfeeding Study was a single-arm open label trial conducted between July 2003 and February 2009. The overall aim was to investigate whether a maternal triple-antiretroviral regimen that was designed to maximally suppress viral load in late pregnancy and the first 6 mo of lactation was a safe, well-tolerated, and effective PMTCT intervention.
Methods and Findings
HIV-infected pregnant women took zidovudine, lamivudine, and either nevirapine or nelfinavir from 34–36 weeks' gestation to 6 mo post partum. Infants received single-dose nevirapine at birth. Women were advised to breastfeed exclusively and wean rapidly just before 6 mo. Using Kaplan-Meier methods we estimated HIV-transmission and death rates from delivery to 24 mo. We compared HIV-transmission rates among subgroups defined by maternal risk factors, including baseline CD4 cell count and viral load.
Conclusions
This trial shows that a maternal triple-antiretroviral regimen from late pregnancy through 6 months of breastfeeding for PMTCT is safe and feasible in a resource-limited setting. These findings are consistent with those from other trials using maternal triple-antiretroviral regimens during breastfeeding in comparable settings.
Trial registration
ClinicalTrials.gov NCT00146380
Please see later in the article for the Editors' Summary
Every year, about half a million children become infected with human immunodeficiency virus (HIV), which causes acquired immunodeficiency syndrome (AIDS). Nearly all these newly infected children live in resource-limited countries and most acquire HIV from their mother, so-called mother-to-child transmission (MTCT). Without intervention, 25%–50% of babies born to HIV-positive mothers become infected with HIV during pregnancy, delivery, or breastfeeding. This infection rate can be reduced by treating mother and child with antiretroviral (ARV) drugs. A single dose of nevirapine (a “non-nucleoside reverse transcriptase inhibitor” or NNRTI) given to the mother at the start of labor and to her baby soon after birth nearly halves the risk of MTCT. Further reductions in risk can be achieved by giving mother and baby three ARVs—an NNRTI and two nucleoside reverse transcriptase inhibitors (NRTIs such as zidovudine and lamivudine)—during pregnancy and perinatally (around the time of birth).
Why Was This Study Done?
Breastfeeding is crucial for child survival in poor countries but it is also responsible for up to half of MTCT. Consequently, many researchers are investigating how various ARV regimens given to mothers and/or their infants during the first few months of life as well as during pregnancy and perinatally affect MTCT. In this single-arm trial, the researchers assess the feasibility and safety of using a triple-ARV regimen to suppress the maternal HIV load (amount of virus in the blood) from late pregnancy though 6 months of breastfeeding among HIV-positive women in Kisumu, Kenya, and ask whether this approach achieves a lower HIV transmission rate than other ARV regimens that have been tested in resource-limited settings. In a single-arm trial, all the participants are given the same treatment. By contrast, in a “randomized controlled” trial, half the participants chosen at random are given the treatment under investigation and the rest are given a control treatment. A randomized controlled trial provides a better comparison of treatments than a single-arm trial but is more costly.
What Did the Researchers Do and Find?
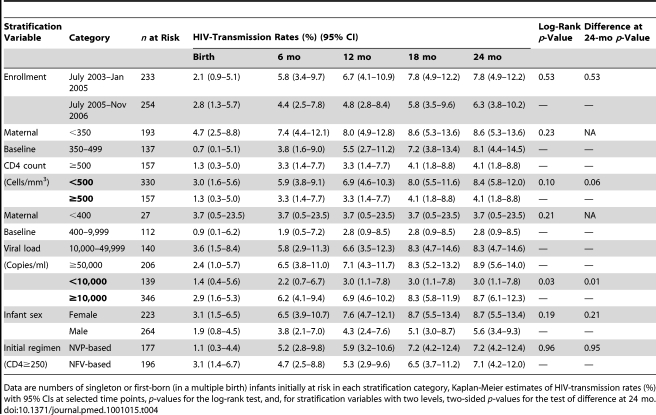
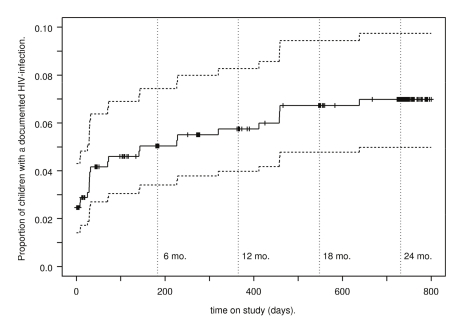
In the Kisumu Breastfeeding Study (KiBS), HIV-infected pregnant women took a triple-ARV regimen containing zidovudine and lamivudine and either nevirapine or the protease inhibitor nelfinavir from 34–36 weeks of pregnancy to 6 months after delivery. They were advised to breastfeed their babies (who received single-dose nevirapine at birth), and to wean them rapidly just before 6 months. The researchers then used Kaplan-Meier statistical methods to estimate HIV transmission and death rates among 487 live-born infants from delivery to 24 months. The cumulative HIV transmission rate rose from 2.5% at birth to 7.0% at 24 months. The cumulative HIV transmission or death rate at 24 months was 15.7%; no infant deaths were attributed to ARVs. At 24 months, 3.0% of babies born to mothers with a low viral load were HIV positive compared to 8.7% of babies born to mothers with a high viral load, a statistically significant difference. Similarly, at 24 months, 8.4% of babies born to mothers with low baseline CD4 cell counts (CD4 cells are immune system cells that are killed by HIV; CD4 cell counts indicate the level of HIV-inflicted immune system damage) were HIV positive compared to 4.1% of babies born to mothers with high baseline CD4 cell counts, although this difference did not achieve statistical significance.
What Do These Findings Mean?
Although these findings are limited by the single-arm design, they support the idea that giving breastfeeding women a triple-ARV regimen from late pregnancy to 6 months is a safe, feasible way to reduce MTCT in resource-limited settings. The HIV transmission rates in this study are comparable to those recorded in similar trials in other resource-limited settings and are lower than MTCT rates observed previously in Kisumu in a study in which no ARVs were used. Importantly, the KiBS mothers took most of the ARVs they were prescribed and most stopped breastfeeding by 6 months as advised. The intense follow-up employed in KiBS may be partly responsible for this good adherence to the trial protocol and thus this study's findings may not be generalizable to all resource-limited settings. Nevertheless, they suggest that a simple triple-ARV regimen given to HIV-positive pregnant women regardless of their baseline CD4 cell count can reduce MTCT during pregnancy and breastfeeding in resource-limited setting.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001015.
-
Subjects:
-
Source:
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files
-

gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
txt 
gif 
jpeg 
gif 
jpeg
txt 
pdf 
doc










More +


 Email
CDC-INFO
Email
CDC-INFO









