
i
HIV-1 Drug Resistance Emergence among Breastfeeding Infants Born to HIV-Infected Mothers during a Single-Arm Trial of Triple-Antiretroviral Prophylaxis for Prevention of Mother-To-Child Transmission: A Secondary Analysis
-
Mar 2011
Source: PLoS Med. 2011; 8(3)
 [PDF-234.12 KB]
[PDF-234.12 KB]
Details:
-
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
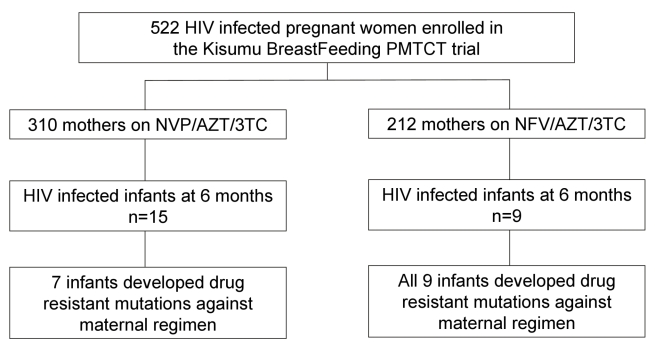
Nevirapine and lamivudine given to mothers are transmitted to infants via breastfeeding in quantities sufficient to have biologic effects on the virus; this may lead to an increased risk of a breastfed infant's development of resistance to maternal antiretrovirals. The Kisumu Breastfeeding Study (KiBS), a single-arm open-label prevention of mother-to-child HIV transmission (PMTCT) trial, assessed the safety and efficacy of zidovudine, lamivudine, and either nevirapine or nelfinavir given to HIV-infected women from 34 wk gestation through 6 mo of breastfeeding. Here, we present findings from a KiBS trial secondary analysis that evaluated the emergence of maternal ARV-associated resistance among 32 HIV-infected breastfed infants.
Methods and Findings
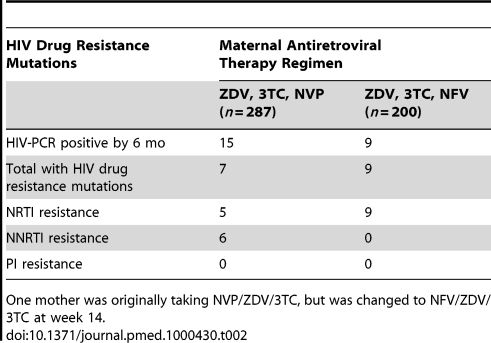
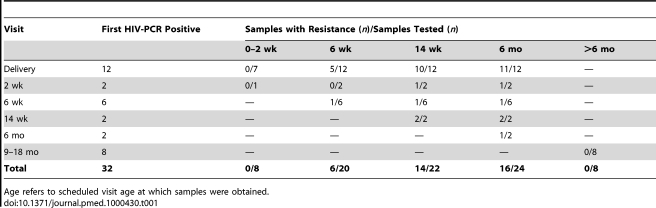
All infants in the cohort were tested for HIV infection using DNA PCR at multiple study visits during the 24 mo of the study, and plasma RNA viral load for all HIV-PCR–positive infants was evaluated retrospectively. Specimens from mothers and infants with viral load >1,000 copies/ml were tested for HIV drug resistance mutations. Overall, 32 infants were HIV infected by 24 mo of age, and of this group, 24 (75%) infants were HIV infected by 6 mo of age. Of the 24 infants infected by 6 mo, nine were born to mothers on a nelfinavir-based regimen, whereas the remaining 15 were born to mothers on a nevirapine-based regimen. All infants were also given single-dose nevirapine within 48 hours of birth. We detected genotypic resistance mutations in none of eight infants who were HIV-PCR positive by 2 wk of age (specimens from six infants were not amplifiable), for 30% (6/20) at 6 wk, 63% (14/22) positive at 14 wk, and 67% (16/24) at 6 mo post partum. Among the 16 infants with resistance mutations by 6 mo post partum, the common mutations were M184V and K103N, conferring resistance to lamivudine and nevirapine, respectively. Genotypic resistance was detected among 9/9 (100%) and 7/15 (47%) infected infants whose mothers were on nelfinavir and nevirapine, respectively. No mutations were detected among the eight infants infected after the breastfeeding period (age 6 mo).
Conclusions
Emergence of HIV drug resistance mutations in HIV-infected infants occurred between 2 wk and 6 mo post partum, most likely because of exposure to maternal ARV drugs through breast milk. Our findings may impact the choice of regimen for ARV treatment of HIV-infected breastfeeding mothers and their infected infants.
Trial Registration
ClinicalTrials.gov NCT00146380
Please see later in the article for the Editors' Summary
Globally, more than 2 million children are infected with the human immunodeficiency virus (HIV) that causes acquired immunodeficiency syndrome (AIDS), and half a million children are newly infected every year. These infections are mainly the result of mother-to-child transmission (MTCT) of HIV during pregnancy, labor and delivery, or through breastfeeding. MTCT can be greatly reduced by treating HIV-positive mothers and their babies with antiretroviral drugs (ARVs). Without ARVs, up to half of babies born to HIV-positive mothers become infected with HIV. This rate of transmission falls to below 5% if a combination of three ARVs is given to the mother throughout pregnancy. Unfortunately, this triple-ARV therapy is too expensive for use in the resource-limited countries where most MTCT occurs. Instead, many such countries have introduced simpler, shorter ARV regimens such as a daily dose of zidovudine (a nucleoside reverse transcriptase inhibitor or NRTI) given to HIV-positive women during late pregnancy coupled with single-dose nevirapine (a non-nucleoside reverse transcriptase inhibitor or NNRTI) at the onset of labor, zidovudine and lamivudine (another NRTI) during labor and delivery, and single-dose nevirapine given to the baby at birth.
Why Was This Study Done?
More than 95% of HIV-exposed children are born in resource-limited settings where breastfeeding is the norm and is crucial for child survival even though it poses a risk of HIV transmission. Consequently, several recent studies have investigated whether MTCT can be further reduced by giving the mother ARVs while she is breastfeeding. In the Kisumu Breastfeeding Study (KiBS), for example, researchers assessed the effects of giving zidovudine, lamivudine, and either nevirapine or nelfinavir (a protease inhibitor) to HIV-infected women from 34 weeks of pregnancy through 6 months of breastfeeding. The results of KiBS indicate that this approach might be a safe, feasible way to reduce MTCT (see the accompanying paper by Thomas and colleagues). However, low amounts of nevirapine and lamivudine are transferred from mother to infant in breast milk and this exposure to ARVs could induce the development of resistance to ARVs among HIV-infected infants. In this KiBS substudy, the researchers investigate whether HIV drug resistance emerged in any of the HIV-positive infants in the parent study.
What Did the Researchers Do and Find?
In KiBS, 32 infants were HIV-positive at 24 months old; 24 were HIV-positive at 6 months old when their mothers stopped taking ARVs and when breastfeeding was supposed to stop. The researchers analyzed blood samples taken from these infants at various ages and from their mothers for the presence of HIV drug resistance mutations (DNA changes that make HIV resistant to killing by ARVs). They detected no resistance mutations in samples taken from 2-week old HIV-positive infants or from the infants who became infected after the age of 6 months. However, they found resistance mutations in a third and two-thirds of samples taken from 6-week and 6-month old HIV-positive infants, respectively. The commonest mutations conferred resistance to lamivudine and nevirapine. Moreover, resistance mutations were present in samples taken from all the HIV-positive infants whose mothers who had received nelfinavir but in only half those taken from infants whose mothers who had received nevirapine. Finally, most of the mothers of HIV-positive infants had no HIV drug resistance mutations, and only one mother-infant pair had an overlapping pattern of HIV drug resistance mutations.
What Do These Findings Mean?
These findings indicate that, in this KiBS substudy, the emergence of HIV drug resistance mutations in HIV-infected infants whose mothers were receiving ARVs occurred between 2 weeks and 6 months after birth. The pattern of mutations suggests that drug resistance most likely arose through exposure of the infants to low levels of ARVs in breast milk rather than through MTCT of drug-resistant virus. These findings need confirming but suggest that infants exposed to ARVs through breast milk—a situation that may become increasingly common given the reduction in MTCT seen in KiBS and other similar trials—should be carefully monitored for HIV infection. Providers should consider the mothers' regimen when choosing treatment for infants who are found to be HIV-infected despite maternal triple drug prophylaxis. Infants exposed to a maternal regimen with NNRTI drugs should receive first-line therapy with lopinavir/ritonavir, a protease inhibitor. The significance of the NRTI mutations such as M184V with regard to response to therapy needs further evaluation. The M184V mutation may result in hypersensitization to other NRTI drugs and delay or reverse zidovudine resistance. Given the limited availability of alternative drugs for infants in resource-limited settings, provision of the standard WHO-recommended first-line NRTI backbone, which includes 3TC, with enhanced monitoring of the infant to ensure virologic suppression, could be considered. Such an approach should reduce both illness and morbidity among infants who become HIV positive through breastfeeding.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/ 10.1371/journal.pmed.1000430.
-
Subjects:
-
Source:
-
Pubmed ID:21468304
-
Pubmed Central ID:PMC3066134
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files
-

gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
xml 
pdf 
gif 
jpeg





More +


 Email
CDC-INFO
Email
CDC-INFO









