
i
Electronic medical record analysis of emergency room visits and hospitalizations in individuals with epilepsy and mental illness comorbidity
-
Jun 25 2015
Source: Epilepsy Behav. 50:55-60. -
Alternative Title:Epilepsy Behav
-
Personal Author:
-
Description:Objective
Epilepsy is a chronic neurological condition that significantly increases risk of injury and premature death. Rates of mental illness are also disproportionately high in those with epilepsy, which can be attributed in part to the stress and stigma associated with epilepsy. Psychiatric conditions generally complicate the management of epilepsy, and understanding how psychiatric comorbidity affects use of crisis-based health resources could inform care approaches that help improve epilepsy care. To better understand effects of psychiatric comorbidity on epilepsy burden, we conducted a 5-year retrospective analysis of data from a large safety-net healthcare network and compared the occurrence of negative health events (NHEs), defined as emergency department (ED) visits and hospitalizations, among individuals with epilepsy and mental illness (E–MI) vs. those with epilepsy alone (E).
Methods
Electronic health record (EHR) data from a large Midwestern U.S. safety-net healthcare system were queried to identify a study population of adults ≥18 years with a diagnosis of epilepsy, with or without mental illness. We assessed demographic and clinical characteristics for each of the 5 years and compared NHEs between subgroups with E–MI vs. E. An additional analysis focused on those individuals who remained in the healthcare system over the entire 5-year study time frame (January, 2010 to December, 2014). Annual and cumulative NHE counts and hospital length of stay for individuals with E–MI and E were assessed, as were hospital discharge diagnoses.
Results
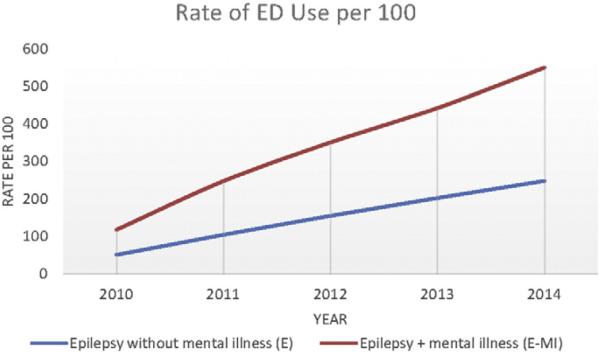
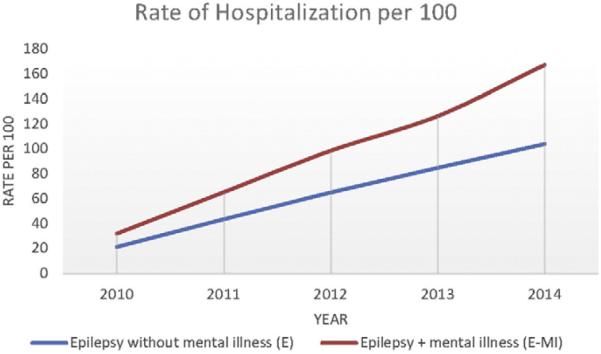
The number (approximately 2000) and demographic characteristics of individuals with epilepsy who received care each year of the study period was relatively consistent. In 2014, mean age of individuals with epilepsy was 48 (range: 18–95), 48.2% were women, 51.5% were White, 37.9% were African-American, and 8.6% were Hispanic. In 2014, there were 1616 (78.6%) individuals in the subgroup with E and 439 (21.4%) in the subgroup with E–MI. Most clinical and demographic variables between the subgroups with E–MI and E were similar, except that individuals with E–MI were less likely to be employed or commercially insured. Overall, NHEs were common, with over 1/4 (27.5%) of all individuals with epilepsy having an ED visit during the year, 13.7% having hospitalization, and 34.2% having either an ED visit or hospitalization. Individuals with E–MI had significantly more NHEs compared to individuals with epilepsy only, as evidenced by higher rates of any NHE (p < .001), ED visits (p < .001), and hospitalizations (p < .001). The cumulative differential in ED and hospital use between subgroups with E–MI and E was substantial over a 5-year time period. While most NHEs were directly related to seizures for the overall group, substance-use complications appeared as a top reason for hospitalization only in the group with E–MI.
Conclusions
Individuals with E–MI made up just over 20% of all people with epilepsy in a safety-net system and had higher rates of NHEs than those without mental illness. Better and earlier identification of individuals with E–MI, assistance with self-management including helping individuals to optimize ambulatory care settings as opposed to the ED, and treatment for substance use disorders could eventually reduce NHEs in this vulnerable subgroup of individuals with epilepsy.
-
Subjects:
-
Source:
-
Pubmed ID:26119621
-
Pubmed Central ID:PMC4793963
-
Document Type:
-
Funding:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
 [PDF-402.73 KB]
[PDF-402.73 KB]
Details:
Supporting Files




More +


 Email
CDC-INFO
Email
CDC-INFO









