
i
Association between Regimen Composition and Treatment Response in Patients with Multidrug-Resistant Tuberculosis: A Prospective Cohort Study
-
Dec 29 2015
Source: PLoS Med. 12(12). -
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
For treating multidrug-resistant tuberculosis (MDR TB), the World Health Organization (WHO) recommends a regimen of at least four second-line drugs that are likely to be effective as well as pyrazinamide. WHO guidelines indicate only marginal benefit for regimens based directly on drug susceptibility testing (DST) results. Recent evidence from isolated cohorts suggests that regimens containing more drugs may be beneficial, and that DST results are predictive of regimen effectiveness. The objective of our study was to gain insight into how regimen design affects treatment response by analyzing the association between time to sputum culture conversion and both the number of potentially effective drugs included in a regimen and the DST results of the drugs in the regimen.
Methods and Findings
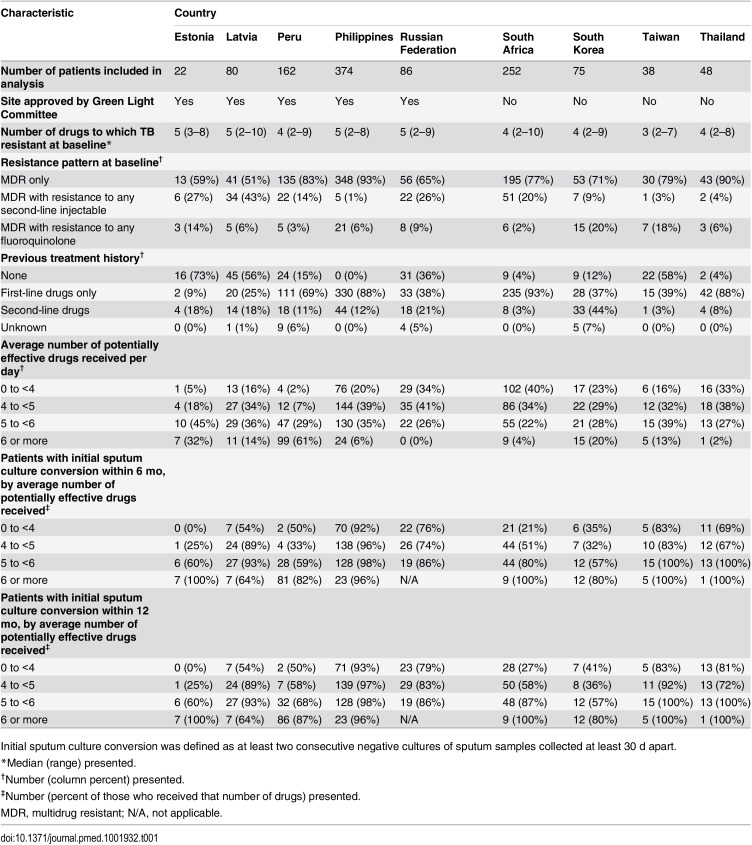
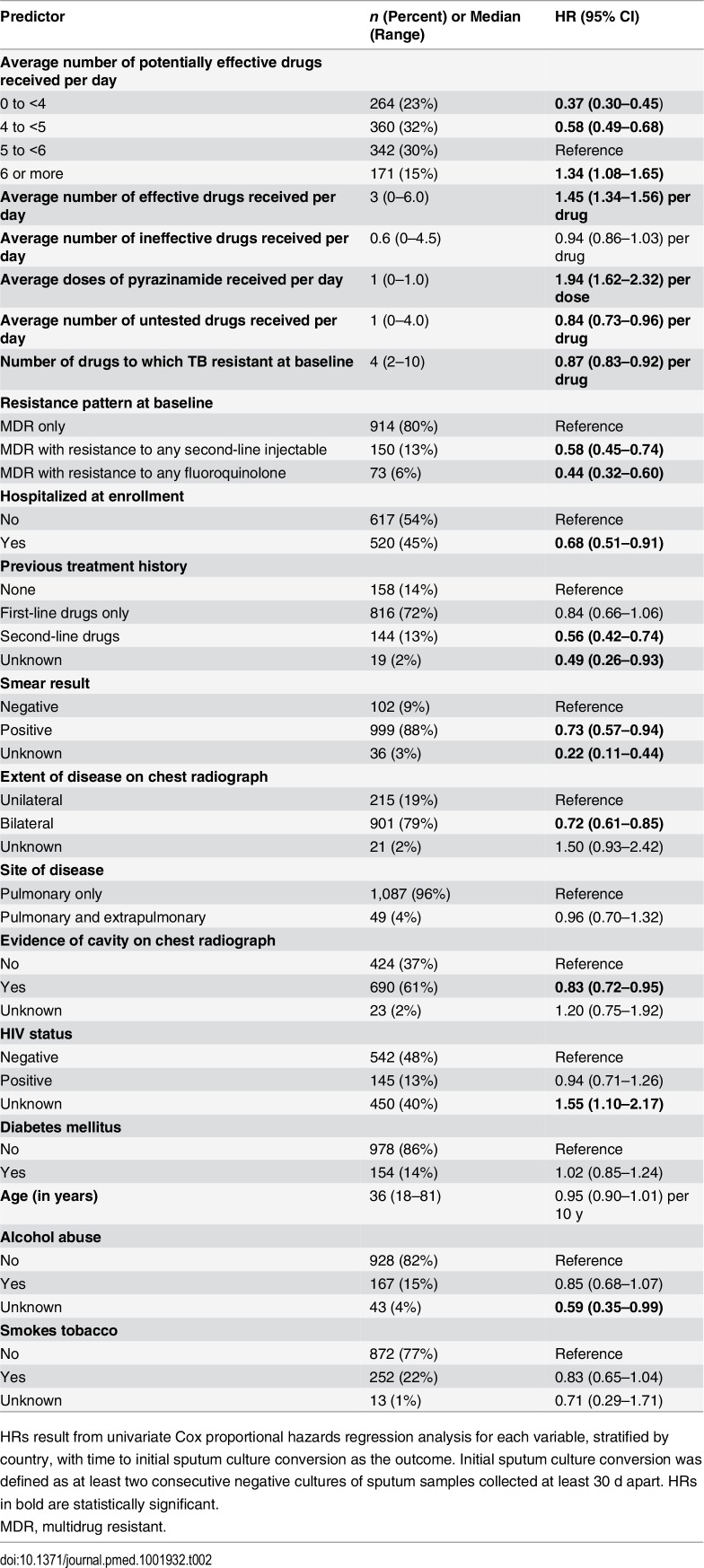
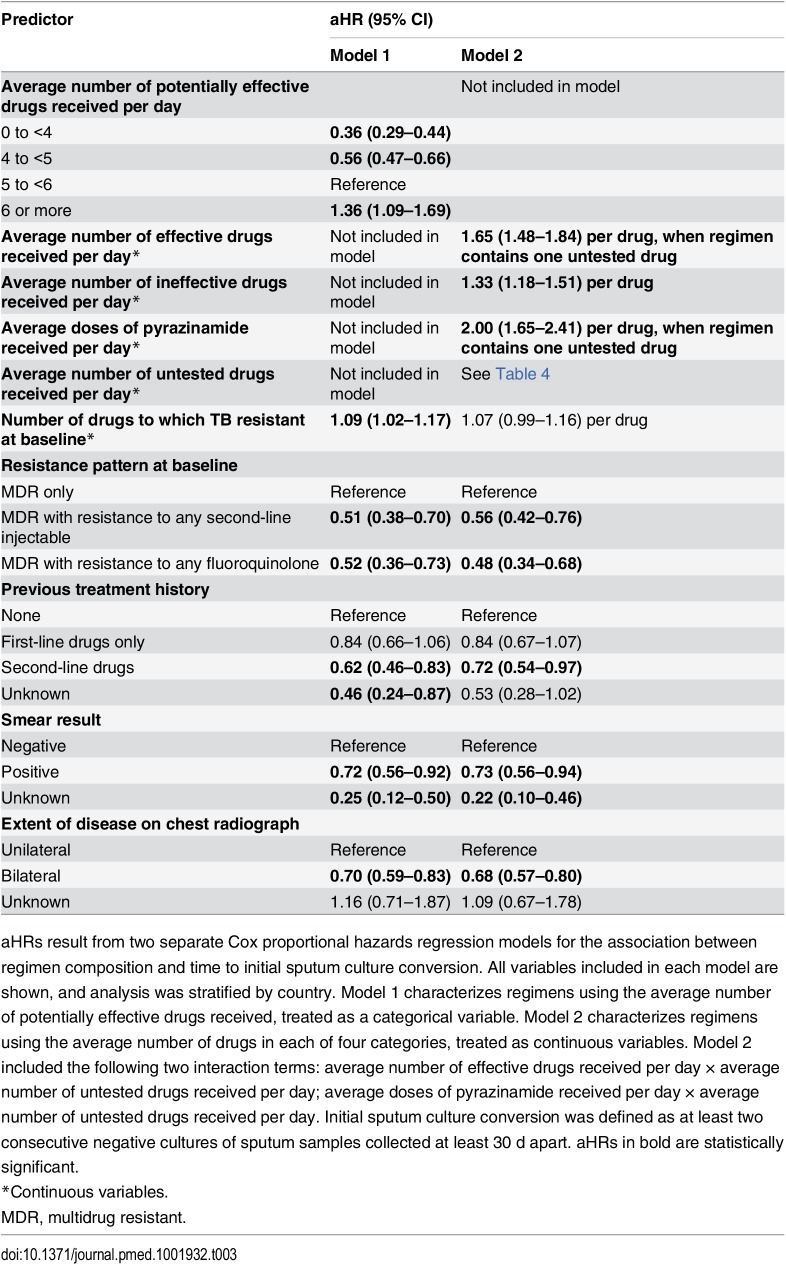
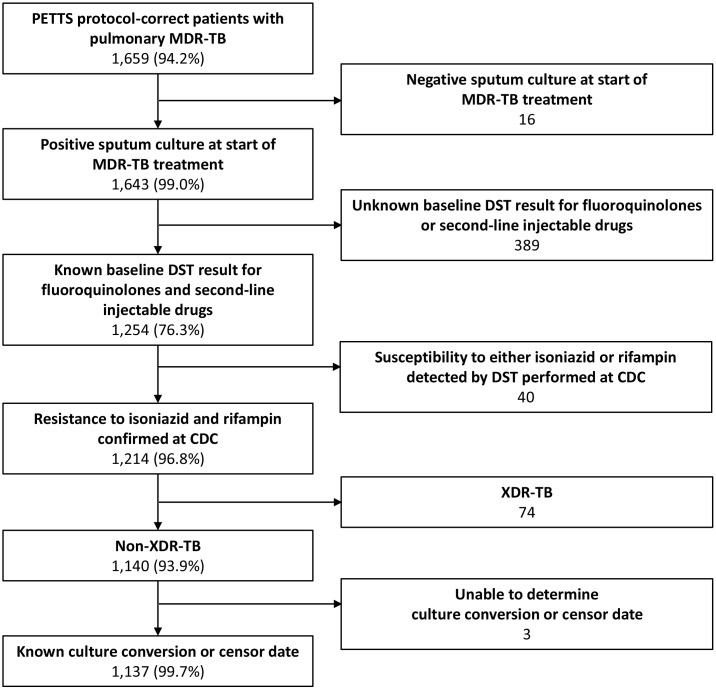
We analyzed data from the Preserving Effective Tuberculosis Treatment Study (PETTS), a prospective observational study of 1,659 adults treated for MDR TB during 2005–2010 in nine countries: Estonia, Latvia, Peru, Philippines, Russian Federation, South Africa, South Korea, Thailand, and Taiwan. For all patients, monthly sputum samples were collected, and DST was performed on baseline isolates at the US Centers for Disease Control and Prevention. We included 1,137 patients in our analysis based on their having known baseline DST results for at least fluoroquinolones and second-line injectable drugs, and not having extensively drug-resistant TB. These patients were followed for a median of 20 mo (interquartile range 16–23 mo) after MDR TB treatment initiation. The primary outcome of interest was initial sputum culture conversion. We used Cox proportional hazards regression, stratifying by country to control for setting-associated confounders, and adjusting for the number of drugs to which patients’ baseline isolates were resistant, baseline resistance pattern, previous treatment history, sputum smear result, and extent of disease on chest radiograph.
Conclusions
MDR TB regimens including more potentially effective drugs than the minimum of five currently recommended by WHO may encourage improved response to treatment in patients with MDR TB. Rapid access to high-quality DST results could facilitate the design of more effective individualized regimens. Randomized controlled trials are necessary to confirm whether individualized regimens with more than five drugs can indeed achieve better cure rates than current recommended regimens.
Background
Tuberculosis (TB)—a contagious bacterial disease that usually infects the lungs—is a global public health problem. The World Health Organization (WHO) estimates that, in 2014, about 9.6 million people developed TB and 1.5 million people died from the disease. Mycobacterium tuberculosis, the organism that causes TB, is spread in airborne droplets when people with TB cough. The symptoms of TB include persistent cough, fever, and weight loss; diagnostic tests for TB include the culture (growth) of M. tuberculosis from sputum samples (mucus coughed up from the lungs) and chest X-rays. TB can be cured by taking several antibiotics (including rifampicin and isoniazid) every day for six months. However, the emergence of multidrug-resistant tuberculosis (MDR TB; TB with resistance to at least both rifampicin and isoniazid) and extensively drug-resistant TB (MDR TB with additional resistance to at least quinolones and to second-line injectable antibiotics) is now threatening TB control efforts—about 5% of the cases of TB that occurred in 2014 were caused by MDR TB.
Why Was This Study Done?
WHO guidelines for the treatment of MDR TB recommend a regimen that includes pyrazinamide and at least four second-line drugs (amikacin or other second-line injectable drugs and fluoroquinolones such as ofloxacin) that are likely to be effective. When bacterial drug susceptibility testing (DST) is not available, determination of the likely effectiveness of drugs is based on patients’ previous exposure to antibiotics and the background drug resistance levels in the community. Although the guidelines state that regimens based on DST results are only marginally more effective than regimens determined without such results, recent evidence suggests that DST results predict regimen effectiveness and that regimens containing more drugs than currently recommended by the guidelines might be beneficial. Here, the researchers undertake a prospective cohort study (an observational study that compares outcomes in non-randomized groups of patients given different treatments) to gain insights into how regimen design affects treatment response among people with MDR TB. Specifically, the researchers analyze the association between both the number of potentially effective drugs included in a regimen and the DST results of the drugs in the regimen and the time to sputum culture conversion (the time between treatment initiation and having two consecutive negative sputum cultures).
What Did the Researchers Do and Find?
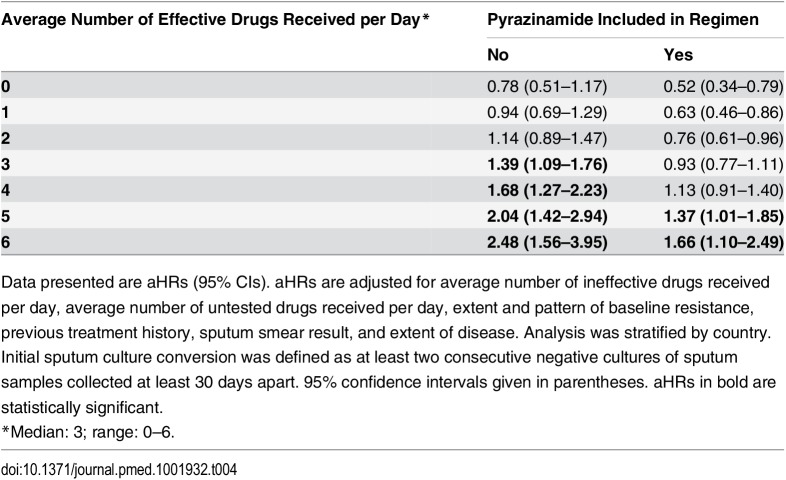
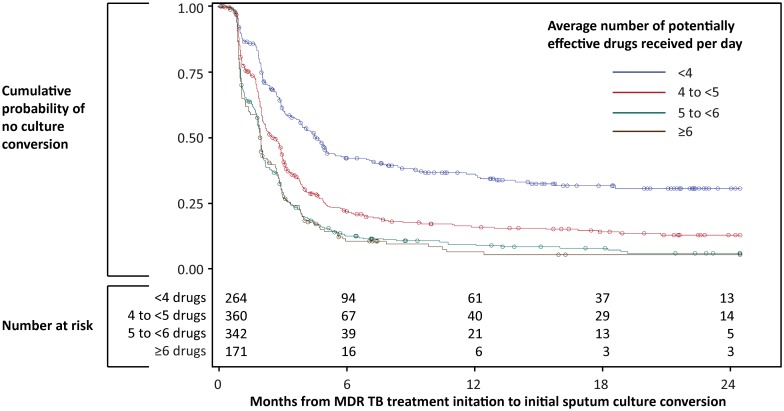
The researchers used a statistical approach called multivariable analysis to analyze data (including baseline DST results and information on the time to sputum culture conversion) collected from 1,137 adults with MDR TB who participated in the Preserving Effective Tuberculosis Treatment Study (PETTS). Receiving an average of at least six potentially effective drugs per day (drugs without a baseline DST result indicating resistance) was associated with a 36% greater likelihood of sputum culture conversion than receiving an average of at least five but fewer than six potentially effective drugs per day. Inclusion of more drugs to which baseline DST results indicated susceptibility was associated with a 65% higher likelihood of sputum culture conversion per drug, and inclusion of pyrazinamide was associated with a doubling of the likelihood of sputum culture conversion, Inclusion of more drugs to which baseline DST results indicated resistance was associated with only a 33% higher likelihood of sputum culture conversion per drug. Finally, inclusion of more drugs for which DST had not been performed was beneficial only if the regimen already contained a minimum of three likely effective drugs.
What Do These Findings Mean?
These findings suggest that regimens that include more potentially effective drugs than currently recommended by WHO might improve the response of patients with MDR TB to treatment. In addition, these findings suggest that rapid access to high-quality DST results could facilitate the design of more effective individualized regimens. However, because this study was based on observational data, these findings do not prove that increasing the number of drugs in treatment regimens or basing drug choice on DST results improves outcomes. It is possible that all the patients who received a particular treatment shared an unknown, non-drug-related characteristic that was actually responsible for their response to treatment. Additionally, the authors were not able to assess the effects of individual drugs, and the analysis assumed equivalent efficacy for all drugs in a particular category, which may not be true in reality. The authors also did not have data on adherence or long-term follow-up to assess relapse or sputum culture reversion. Thus, although these findings suggest that changes to the current WHO guidelines for the treatment of MDR TB might be beneficial, randomized controlled trials should be undertaken first to confirm whether individualized regimens that include more than five drugs can achieve better cure rates than the currently recommended regimens.
Additional Information
This list of resources contains links that can be accessed when viewing the PDF on a device or via the online version of the article at http://dx.doi.org/10.1371/journal.pmed.1001932.
-
Subjects:
-
Source:
-
Pubmed ID:26714320
-
Pubmed Central ID:PMC4700973
-
Document Type:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-

pdf 
pdf 
pdf 
pdf 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
txt 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
bin 
pdf 
pdf
 [PDF-528.88 KB]
[PDF-528.88 KB]
Details:
Supporting Files





More +
You May Also Like

 [PDF - 41.14 KB]
[PDF - 41.14 KB]
 Email
CDC-INFO
Email
CDC-INFO









