
i
Improving documentation and coding for acute organ dysfunction biases estimates of changing sepsis severity and burden: a retrospective study
-
Sep 14 2015
Source: Crit Care. 19(1). -
Alternative Title:Crit Care
-
Personal Author:
-
Corporate Authors:
-
Description:Introduction
Claims-based analyses report that the incidence of sepsis-associated organ dysfunction is increasing. We examined whether coding practices for acute organ dysfunction are changing over time and if so, whether this is biasing estimates of rising severe sepsis incidence and severity.
Methods
We assessed trends from 2005 to 2013 in the annual sensitivity and incidence of discharge ICD-9-CM codes for organ dysfunction (shock, respiratory failure, acute kidney failure, acidosis, hepatitis, coagulopathy, and thrombocytopenia) relative to standardized clinical criteria (use of vasopressors/inotropes, mechanical ventilation for ≥2 consecutive days, rise in baseline creatinine, low pH, elevated transaminases or bilirubin, abnormal international normalized ratio or low fibrinogen, and decline in platelets). We studied all adult patients with suspected infection (defined by ≥1 blood culture order) at two US academic hospitals.
Results
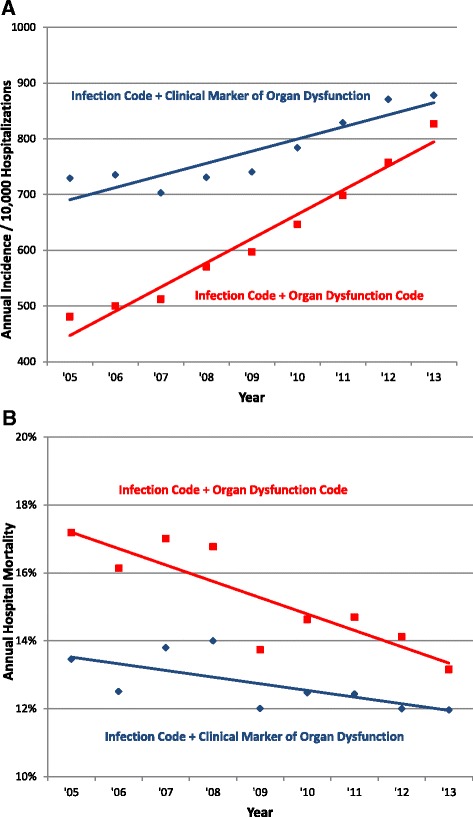
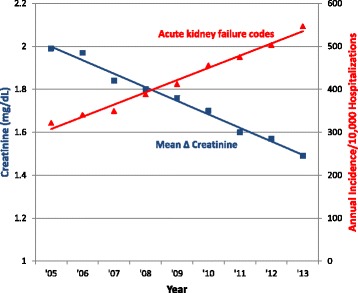
Acute organ dysfunction codes were present in 57,273 of 191,695 (29.9 %) hospitalizations with suspected infection, most commonly acute kidney failure (60.2 % of cases) and respiratory failure (28.9 %). The sensitivity of all organ dysfunction codes except thrombocytopenia increased significantly over time. This was most pronounced for acute kidney failure codes, which increased in sensitivity from 59.3 % in 2005 to 87.5 % in 2013 relative to a fixed definition for changes in creatinine (p = 0.019 for linear trend). Acute kidney failure codes were increasingly assigned to patients with smaller creatinine changes: the average peak creatinine change associated with a code was 1.99 mg/dL in 2005 versus 1.49 mg/dL in 2013 (p <0.001 for linear decline). The mean number of dysfunctional organs in patients with suspected infection increased from 0.32 to 0.59 using discharge codes versus 0.69 to 0.79 using clinical criteria (p <0.001 for both trends and comparison of the two trends). The annual incidence of hospitalizations with suspected infection and any dysfunctional organ rose an average of 5.9 % per year (95 % CI 4.3, 7.4 %) using discharge codes versus only 1.1 % (95 % CI 0.1, 2.0 %) using clinical criteria.
Conclusions
Coding for acute organ dysfunction is becoming increasingly sensitive and the clinical threshold to code patients for certain kinds of organ dysfunction is decreasing. This accounts for much of the apparent rise in severe sepsis incidence and severity imputed from claims.
-
Subjects:
-
Source:
-
Pubmed ID:26369326
-
Pubmed Central ID:PMC4570698
-
Document Type:
-
Funding:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-
gif
jpeg 
txt
txt
gif
jpeg
gif
jpeg
gif
jpeg
 [PDF-1.30 MB]
[PDF-1.30 MB]
Details:
Supporting Files



More +


 Email
CDC-INFO
Email
CDC-INFO









