
i
Description of 3,180 Courses of Chelation with Dimercaptosuccinic Acid in Children ≤5 y with Severe Lead Poisoning in Zamfara, Northern Nigeria: A Retrospective Analysis of Programme Data
-
Oct 07 2014
Source: PLoS Med. 2014; 11(10). -
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Jane Greig and colleagues from the medical humanitarian organization Médecins Sans Frontières describe the use of the oral chelating agent dimercaptosuccinic acid (DMSA) in several thousand young children with severe lead poisoning as a result of an environmental disaster in Zamfara, northern Nigeria.
Background
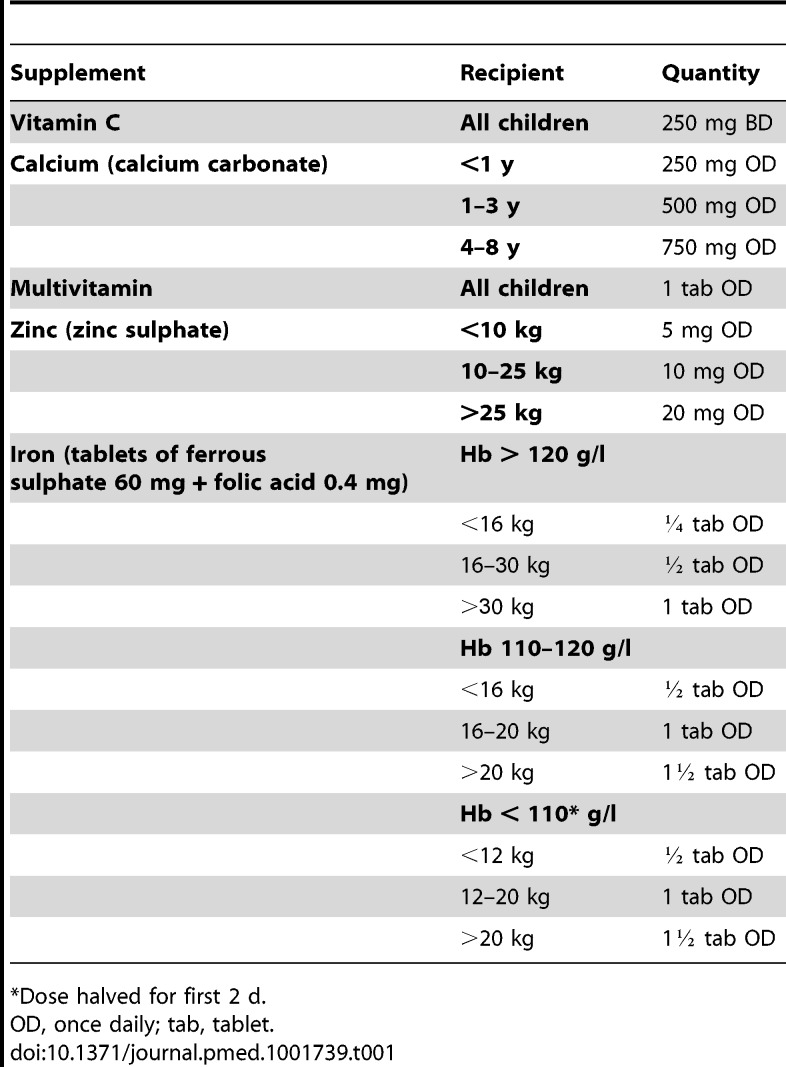
In 2010, Médecins Sans Frontières (MSF) discovered extensive lead poisoning impacting several thousand children in rural northern Nigeria. An estimated 400 fatalities had occurred over 3 mo. The US Centers for Disease Control and Prevention (CDC) confirmed widespread contamination from lead-rich ore being processed for gold, and environmental management was begun. MSF commenced a medical management programme that included treatment with the oral chelating agent 2,3-dimercaptosuccinic acid (DMSA, succimer). Here we describe and evaluate the changes in venous blood lead level (VBLL) associated with DMSA treatment in the largest cohort of children ≤5 y of age with severe paediatric lead intoxication reported to date to our knowledge.
Methods and Findings
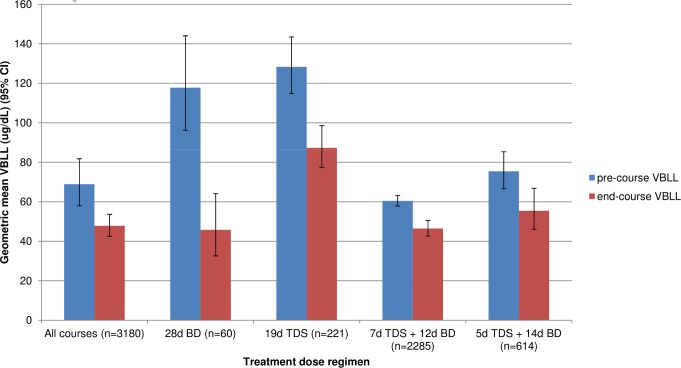
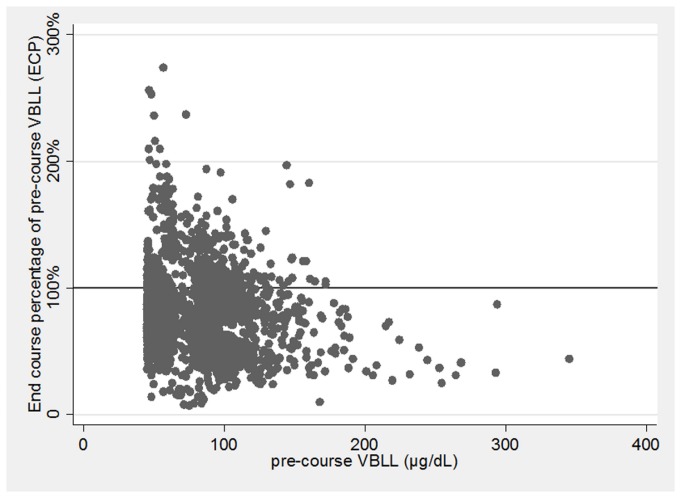
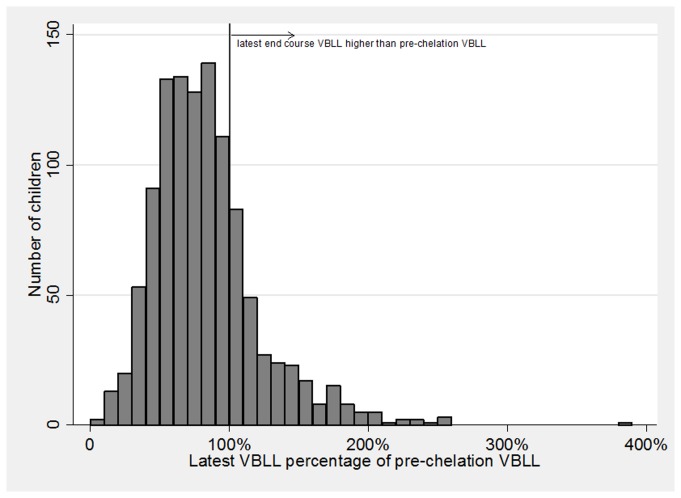
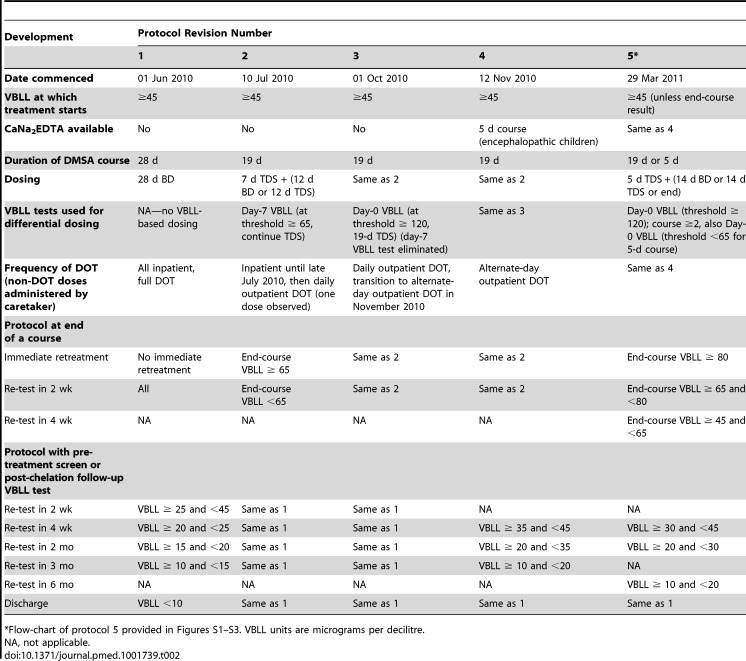
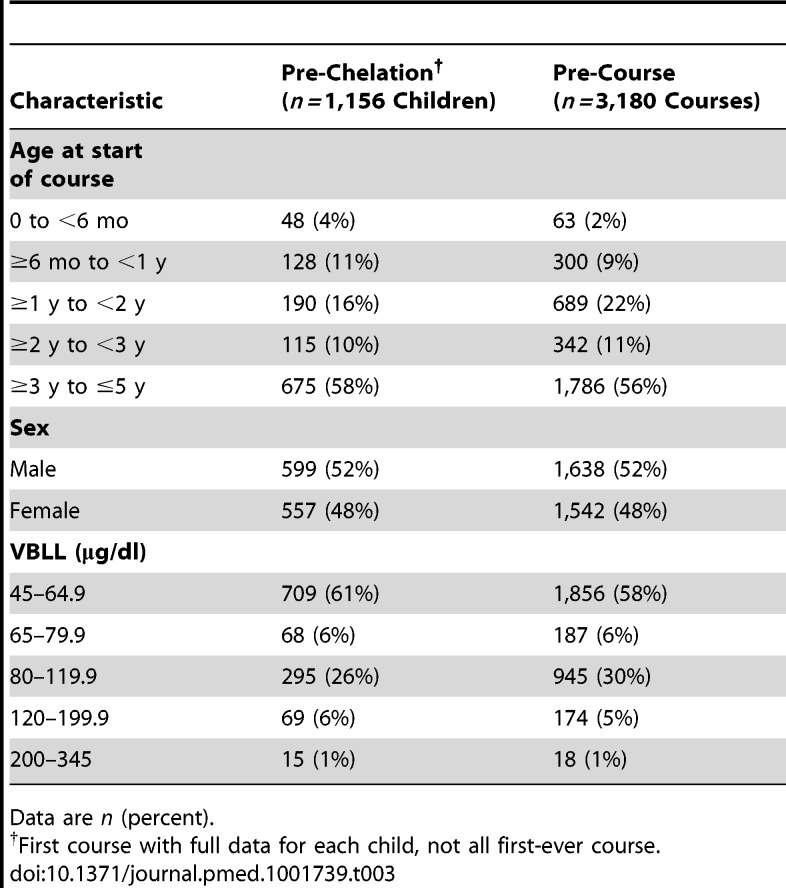
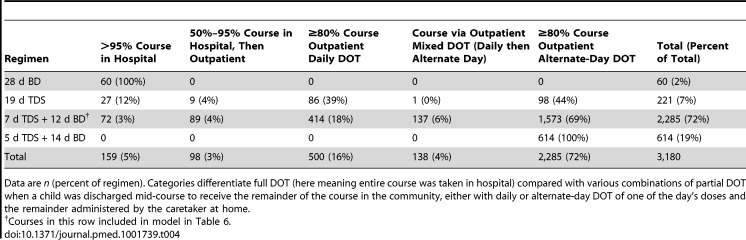
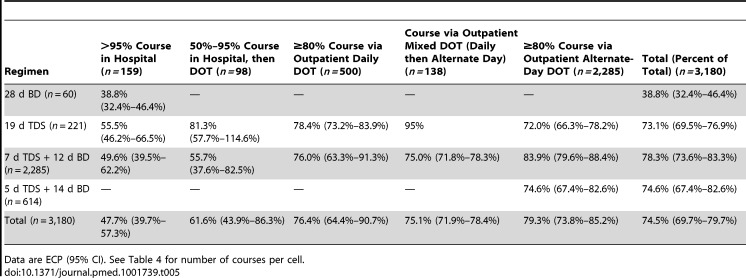
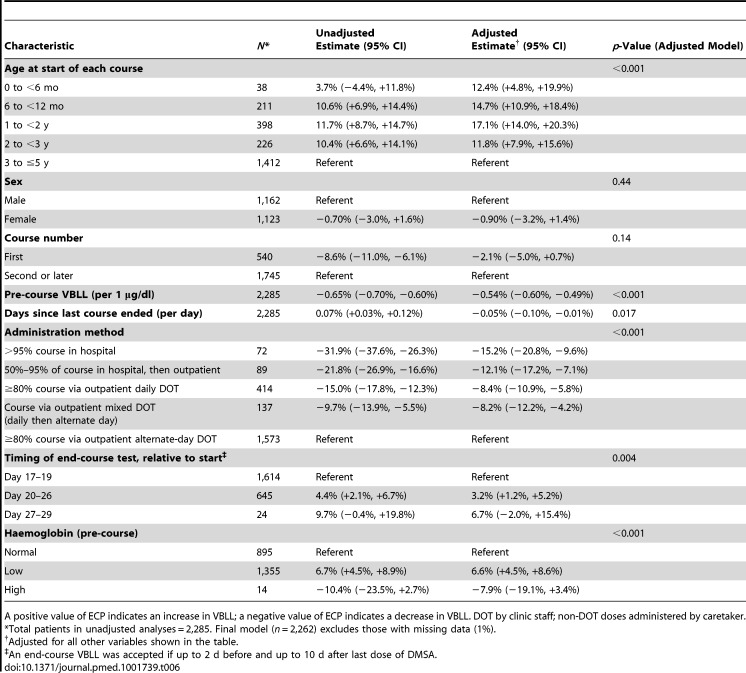
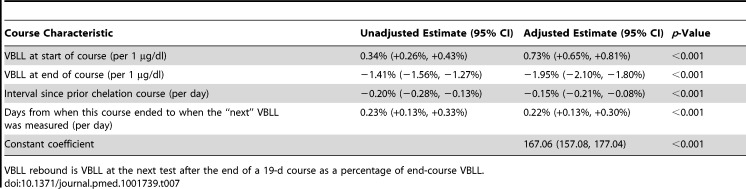
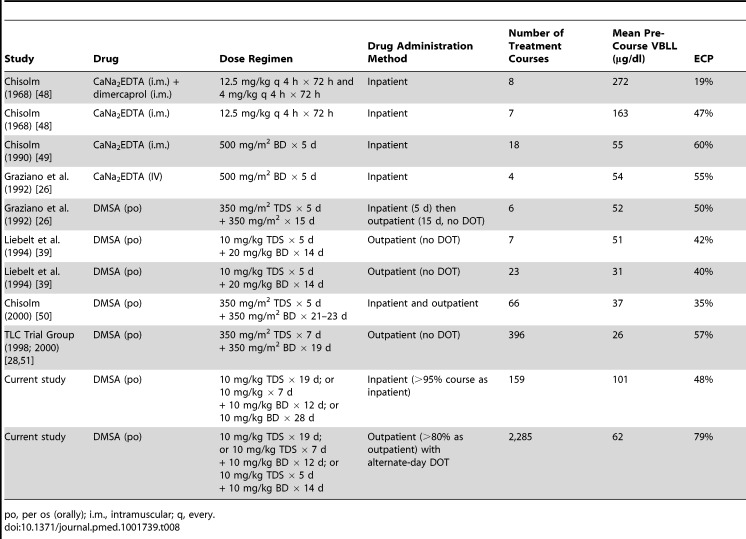
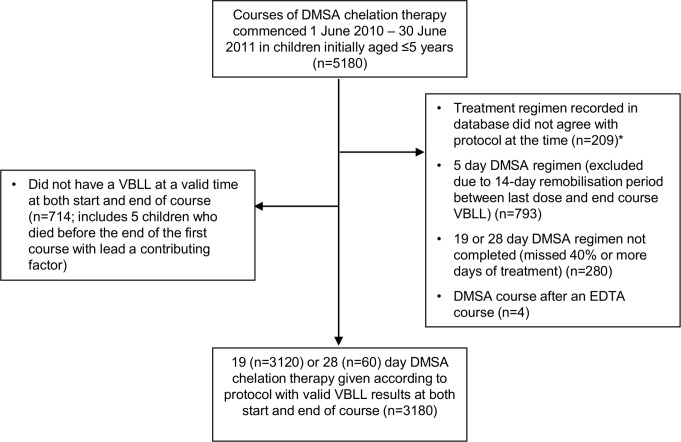
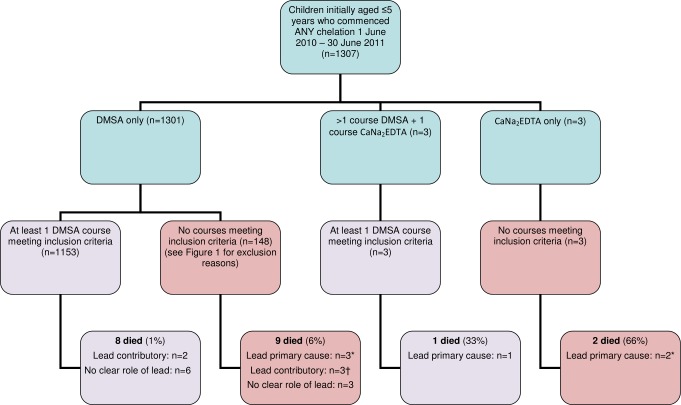
In a retrospective analysis of programme data, we describe change in VBLL after DMSA treatment courses in a cohort of 1,156 children ≤5 y of age who underwent between one and 15 courses of chelation treatment. Courses of DMSA of 19 or 28 d duration administered to children with VBLL ≥ 45 µg/dl were included. Impact of DMSA was calculated as end-course VBLL as a percentage of pre-course VBLL (ECP). Mixed model regression with nested random effects was used to evaluate the relative associations of covariates with ECP. Of 3,180 treatment courses administered, 36% and 6% of courses commenced with VBLL ≥ 80 µg/dl and ≥ 120 µg/dl, respectively. Overall mean ECP was 74.5% (95% CI 69.7%–79.7%); among 159 inpatient courses, ECP was 47.7% (95% CI 39.7%–57.3%). ECP after 19-d courses (n = 2,262) was lower in older children, first-ever courses, courses with a longer interval since a previous course, courses with more directly observed doses, and courses with higher pre-course VBLLs. Low haemoglobin was associated with higher ECP. Twenty children aged ≤5 y who commenced chelation died during the period studied, with lead poisoning a primary factor in six deaths. Monitoring of alanine transaminase (ALT), creatinine, and full blood count revealed moderate ALT elevation in <2.5% of courses. No clinically severe adverse drug effects were observed, and no laboratory findings required discontinuation of treatment. Limitations include that this was a retrospective analysis of clinical data, and unmeasured variables related to environmental exposures could not be accounted for.
Conclusions
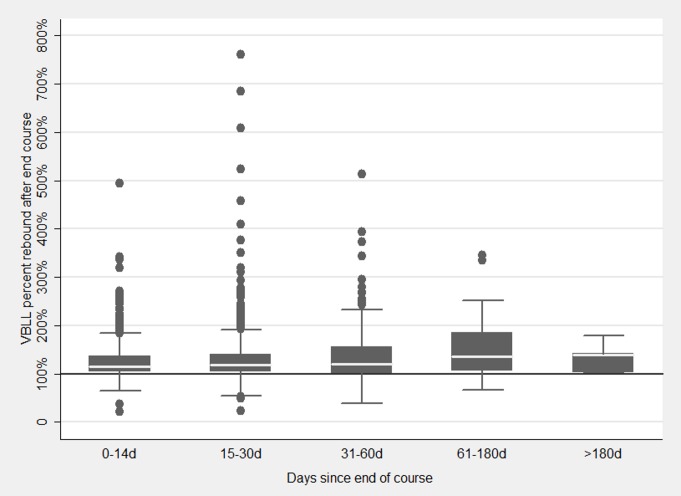
Oral DMSA was a pharmacodynamically effective chelating agent for the treatment of severe childhood lead poisoning in a resource-limited setting. Re-exposure to lead, despite efforts to remediate the environment, and non-adherence may have influenced the impact of outpatient treatment.
Lead, a toxic metal that occurs naturally in the earth's crust, is now present throughout the environment because of human activities. For many years, lead was added to paint and gasoline and used in solder for water pipes. In addition, the mining, smelting, and refining of some metallic ores releases lead into the environment. Inhalation of contaminated air, consumption of contaminated food and water, and contact with dust that contains lead raises venous blood lead levels (VBLLs) and causes many health problems, particularly in children. Children who ingest large amounts of lead can develop anemia, muscle weakness, kidney damage, and life-threatening encephalopathy (brain swelling). Although fatal lead poisoning is now rare in resource-rich countries, it nevertheless remains a major global health problem. Over a three-month period in early 2010, for example, about 400 young children died in Zamfara State, Nigeria, from unexplained, intractable fits. By May 2010, it was clear that recently expanded gold mining had caused widespread environmental lead contamination in the region, and an environmental management program was begun to reduce lead levels in the surface soils.
Why Was This Study Done?
In response to the lead poisoning outbreak, the not-for-profit organization Médecins Sans Frontières (MSF) began a medical management program to reduce VBLLs that included treatment with the oral chelation agent dimercaptosuccinic acid (DMSA). Chelation agents bind metal ions and facilitate their removal from the body, thereby reducing the likelihood of lead moving from the blood to the brain. Lead encephalopathy has been commonly treated by injecting another chelator called CaNa2EDTA, but the discovery of more than 1,000 cases of childhood lead poisoning in rural villages in Nigeria meant that MSF needed a chelation approach that could be applied rapidly in a remote resource-limited setting. Additionally, although CaNa2EDTA has been in common use for severe lead poisoning for longer than DMSA, and is commonly recommended in guidelines, the evidence base does not support one treatment as superior. Here, in a retrospective analysis of MSF program data, the researchers evaluate the changes in VBLLs before and after courses of oral DMSA treatment in children aged five years and below living in Zamfara to gain new insights into this understudied treatment for severe childhood lead poisoning.
What Did the Researchers Do and Find?
The researchers measured VBLLs before and after treatment with DMSA in 1,156 children (inpatient and outpatient) with high amounts of lead in their blood who underwent one or more courses of chelation treatment lasting 19 or 28 days by calculating each child's end-course VBLL as a percentage of the child's pre-course VBLL (ECP). Considering all the treatment courses given between June 2010 and June 2011, the mean (average) ECP was 74.5%. That is, on average, VBLLs measured at the end of treatment courses were reduced by a quarter compared to VBLLs at the start of treatment courses. Among 159 inpatient courses of DMSA, the ECP was 47.7% (a halving of pre-course VBLLs). The ECP after 19-day courses was lower in older children, after first-ever courses, after courses with a longer interval since a previous course, after courses that included more directly observed doses (DMSA given in the presence of a health-care worker), and in children with higher pre-course VBLLs. Nine of the children included in this analysis died during the study period; lead poisoning was probably involved in three of these deaths. Importantly, no clinically severe adverse effects related to DMSA were seen during the study period, and no laboratory findings were recorded that required treatment discontinuation.
What Do These Findings Mean?
Because many changes were made to the treatment given to the affected children in Zamfara during the study period and because no information is presented here on clinical outcomes, these findings cannot be used to reach any definitive conclusions about the effectiveness or safety of oral DMSA as a treatment for lead poisoning in young children. However, these findings show that chelation was associated with a large reduction in the death rate among probable or suspected cases of childhood lead poisoning in Zamfara and provide new information about oral chelation that may help agencies such as MSF provide urgent treatment for lead poisoning in resource-limited settings where intravenous chelation is not feasible. Moreover, the finding of a lower ECP after inpatient treatment courses compared to after outpatient courses suggests that re-exposure to lead and non-adherence to treatment may have influenced the impact of outpatient treatments. Thus, it is essential that medical management of lead poisoning in resource-limited settings be accompanied by environmental remediation and that efforts are made to support adherence to treatment in the community by implementing directly observed treatment wherever possible.
Additional Information
Please access these websites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001739.
-
Subjects:
-
Source:
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-
jpeg
gif
jpeg
gif
jpeg
gif
jpeg 
txt
tiff
tiff
txt
tiff
doc
gif
jpeg
gif
jpeg
gif
jpeg
gif
jpeg
gif
gif
jpeg
gif
jpeg
gif
jpeg
gif
jpeg
jpeg
gif
jpeg
gif
jpeg
gif
 [PDF-1.20 MB]
[PDF-1.20 MB]
Details:
Supporting Files





More +


 Email
CDC-INFO
Email
CDC-INFO









