
i
Removing the Age Restrictions for Rotavirus Vaccination: A Benefit-Risk Modeling Analysis
-
Oct 23 2012
Source: PLoS Med. 2012; 9(10).
 [PDF-762.04 KB]
[PDF-762.04 KB]
Details:
-
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Background
To minimize potential risk of intussusception, the World Health Organization (WHO) recommended in 2009 that rotavirus immunization should be initiated by age 15 weeks and completed before 32 weeks. These restrictions could adversely impact vaccination coverage and thereby its health impact, particularly in developing countries where delays in vaccination often occur.
Methods and Findings
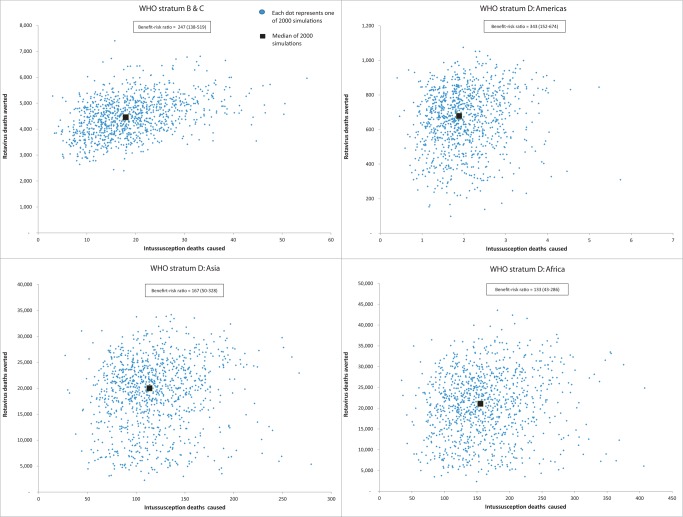
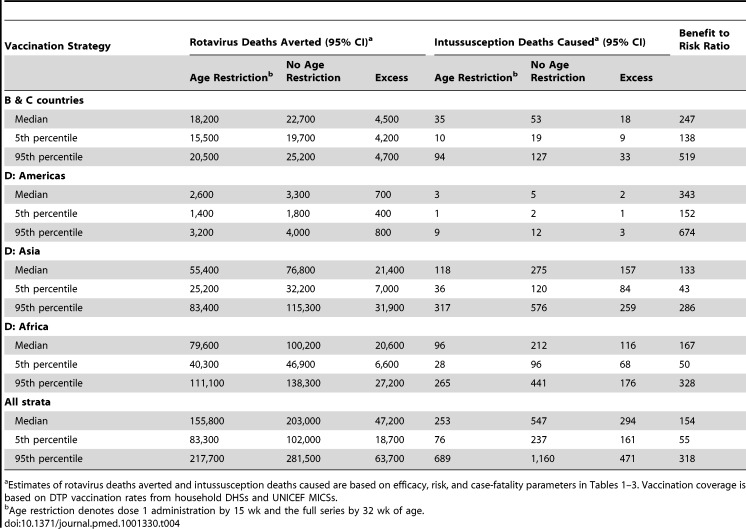
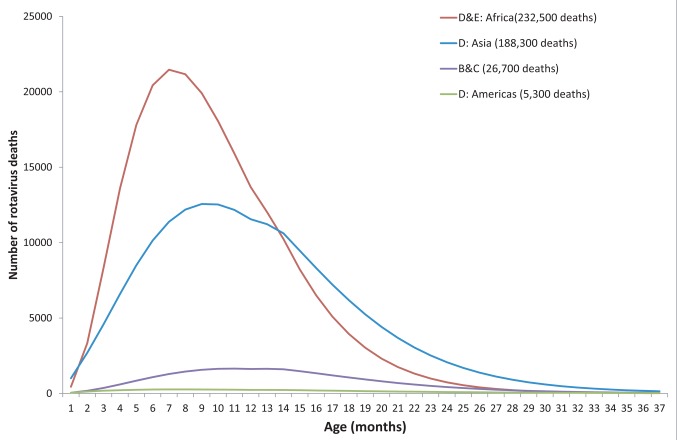
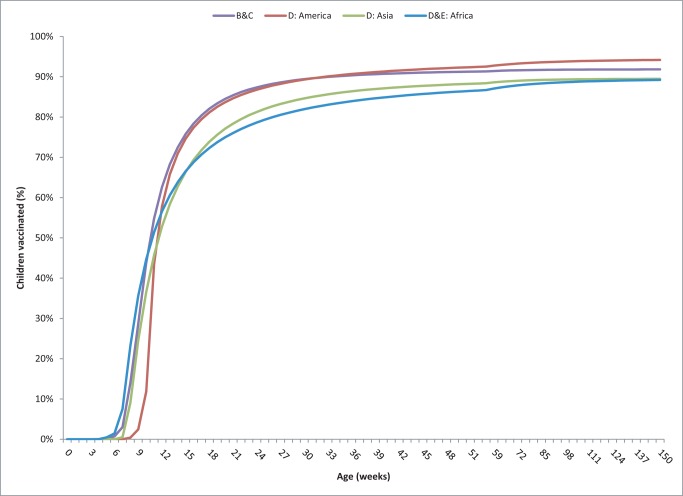
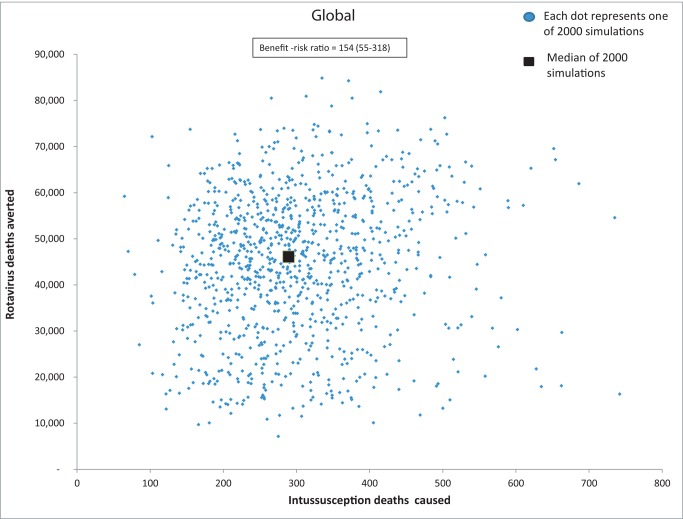
We conducted a modeling study to estimate the number of rotavirus deaths prevented and the number of intussusception deaths caused by vaccination when administered on the restricted schedule versus an unrestricted schedule whereby rotavirus vaccine would be administered with DTP vaccine up to age 3 years. Countries were grouped on the basis of child mortality rates, using WHO data. Inputs were estimates of WHO rotavirus mortality by week of age from a recent study, intussusception mortality based on a literature review, predicted vaccination rates by week of age from USAID Demographic and Health Surveys, the United Nations Children's Fund (UNICEF) Multiple Indicator Cluster Surveys (MICS), and WHO-UNICEF 2010 country-specific coverage estimates, and published estimates of vaccine efficacy and vaccine-associated intussusception risk. On the basis of the error estimates and distributions for model inputs, we conducted 2,000 simulations to obtain median estimates of deaths averted and caused as well as the uncertainty ranges, defined as the 5th–95th percentile, to provide an indication of the uncertainty in the estimates.
Conclusions
Our analysis suggests that in low- and middle-income countries the additional lives saved by removing age restrictions for rotavirus vaccination would far outnumber the potential excess vaccine-associated intussusception deaths.
Rotavirus causes severe diarrhea and vomiting. It is responsible for a large number of hospitalizations among young children in developed countries (an estimated 60,000 hospitalizations per year in the US in 2005, for example). In poor countries, rotavirus is a major cause of death in children under five. In 1998, the first rotavirus vaccine, called RotaShield, was approved in the US by the Food and Drug Administration. Shortly after the vaccine became widely used, doctors noticed a small increase in a problem called intussusception among the vaccinated infants. Intussusception is a rare type of bowel obstruction that occurs when the bowel telescopes in on itself. Prompt treatment of intussusception normally leads to full recovery, but some children with the condition need surgery, and when the disease is left untreated it can be fatal. Because intussusception is a serious condition and because very few children die from rotavirus infection in the United States, the US authorities stopped recommending vaccination with RotaShield in 1999. The manufacturer withdrew the vaccine from the market shortly thereafter.
Why Was This Study Done?
Since 2006, hundreds of thousands of infants have been vaccinated with Rotarix or RotaTeq, with safety being closely monitored. Some countries have reported a small increase in intussusception (one to four additional cases per 100,000 vaccinated infants, compared with one per 2,000 of cases that occur in unvaccinated children). This increase is much lower than the one seen previously with RotaShield. In response to these findings, authorities in the US and other developed countries as well as the World Health Organization declared that the benefits of the vaccine outweigh the risks of the small number of additional intussusception cases in both developed and poor countries. However, because older infants have a higher risk of naturally occurring intussusception, they decided that the course of vaccination (three oral doses for Rotarix and two for RotaTeq) should be initiated before 15 weeks of age and completed before the age of 32 weeks. This is usually not a problem in countries with easy access to health facilities. However, in many poor countries where delays in infant vaccination are common, giving the vaccine only to very young children means that many others who could benefit from its protection will be excluded. In this study, the researchers examined the risks and benefits of rotavirus vaccination in poor countries where most of the rotavirus deaths occur. Specifically, they looked at the benefits and risks if the age restrictions were removed, with a particular emphasis on allowing infants to initiate rotavirus immunization even if they arrive after 15 weeks of age.
What Did the Researchers Do and Find?
The researchers used the most recent estimates for how well the vaccines protect children in Africa and Asia from becoming infected with rotavirus, how many deaths from rotavirus infection can be avoided by vaccination, how many additional cases of intussusception will likely occur in vaccinated children, and what proportion of children would be excluded from rotavirus vaccination because they are too old when they come to a health facility for their infant vaccination. They then estimated the number of rotavirus deaths prevented and the number of intussusception deaths caused by vaccination in two scenarios. The first one (the restricted scenario) corresponds to previous guidelines from WHO and others, in which rotavirus vaccination needs to be initiated before 15 weeks and the full series completed before 32 weeks. The second one (called the unrestricted scenario) allows rotavirus vaccination of children alongside current routinely administered vaccines up to three years of age, recognizing that most children receive their vaccination by 1 year of life.
What Do These Findings Mean?
If one accepts that deaths caused by a vaccine are not fundamentally different from deaths caused by a failure to vaccinate, then these results show that the benefits of lifting the age restriction for rotavirus vaccine clearly outweigh the risks, at least when only examining mortality outcomes. The calculations are valid only for low-income countries in Africa and Asia where both vaccination delays and deaths from rotavirus are common. The risk-benefit ratio will be different elsewhere. There are also additional risks and benefits that are not included in the study's estimates. For example, early vaccination might be seen as less of an urgent priority when this vaccine can be had at a later date, leaving very young children more vulnerable. On the other hand, when many children in the community are vaccinated, even the unvaccinated children are less likely to get infected (what is known as “herd immunity”), something that has not been taken into account in the benefits here. The results of this study (and its limitations) were reviewed in April 2012 by WHO's Strategic Advisory Group of Experts. The group then recommended that, while early vaccination is still strongly encouraged, the age restriction on rotavirus vaccination should be removed in countries where delays in vaccination and rotavirus mortality are common so that more vulnerable children can be vaccinated and deaths from rotavirus averted.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001330.
-
Subjects:
-
Source:
-
Document Type:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
Supporting Files
-

jpeg 
txt 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg
txt 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif 
jpeg 
gif






More +


 Email
CDC-INFO
Email
CDC-INFO









