
i
Adherence to Antiretroviral Prophylaxis for HIV Prevention: A Substudy Cohort within a Clinical Trial of Serodiscordant Couples in East Africa
-
Sep 10 2013
Source: PLoS Med. 2013; 10(9). -
Alternative Title:PLoS Med
-
Personal Author:
-
Description:Jessica Haberer and colleagues investigate the association between high adherence to antiretroviral pre-exposure prophylaxis and HIV transmission in a substudy of serodiscordant couples participating in a clinical trial.
Background
Randomized clinical trials of oral antiretroviral pre-exposure prophylaxis (PrEP) for HIV prevention have widely divergent efficacy estimates, ranging from 0% to 75%. These discrepancies are likely due to differences in adherence. To our knowledge, no studies to date have examined the impact of improving adherence through monitoring and/or intervention, which may increase PrEP efficacy, or reported on objective behavioral measures of adherence, which can inform PrEP effectiveness and implementation.
Methods and Findings
Within the Partners PrEP Study (a randomized placebo-controlled trial of oral tenofovir and emtricitabine/tenofovir among HIV-uninfected members of serodiscordant couples in Kenya and Uganda), we collected objective measures of PrEP adherence using unannounced home-based pill counts and electronic pill bottle monitoring. Participants received individual and couples-based adherence counseling at PrEP initiation and throughout the study; counseling was intensified if unannounced pill count adherence fell to <80%. Participants were followed monthly to provide study medication, adherence counseling, and HIV testing. A total of 1,147 HIV-uninfected participants were enrolled: 53% were male, median age was 34 years, and median partnership duration was 8.5 years. Fourteen HIV infections occurred among adherence study participants—all of whom were assigned to placebo (PrEP efficacy = 100%, 95% confidence interval 83.7%–100%, p<0.001). Median adherence was 99.1% (interquartile range [IQR] 96.9%–100%) by unannounced pill counts and 97.2% (90.6%–100%) by electronic monitoring over 807 person-years. Report of no sex or sex with another person besides the study partner, younger age, and heavy alcohol use were associated with <80% adherence; the first 6 months of PrEP use and polygamous marriage were associated with >80% adherence. Study limitations include potential shortcomings of the adherence measures and use of a convenience sample within the substudy cohort.
Conclusions
The high PrEP adherence achieved in the setting of active adherence monitoring and counseling support was associated with a high degree of protection from HIV acquisition by the HIV-uninfected partner in heterosexual serodiscordant couples. Low PrEP adherence was associated with sexual behavior, alcohol use, younger age, and length of PrEP use.
Every year, about 2.5 million people (mostly living in sub-Saharan Africa) become infected with HIV, the virus that causes AIDS. HIV, which is usually transmitted through unprotected sex with an HIV-infected partner, destroys immune system cells, leaving infected individuals susceptible to other infections. There is no cure for AIDS, although antiretroviral drugs can hold HIV in check, and there is no vaccine against HIV infection. Individuals can reduce their risk of HIV infection by abstaining from sex, by having only one or a few low risk sexual partners, and by always using a condom. In addition, antiretroviral drugs can potentially be used in two ways to reduce HIV transmission. First, these drugs could be given to HIV-positive individuals to reduce their infectiousness. Second, antiretroviral drugs could be given to HIV-uninfected people to reduce acquisition of the virus. This approach—pre-exposure prophylaxis (PrEP)—has provided varying levels of protection against HIV infection in randomized controlled trials (RCT; studies that monitor the outcomes of groups of patients randomly assigned to receive different test drugs or a placebo/dummy drug).
Why Was This Study Done?
One hypothesis for the varying efficacy of PrEP in RCTs is differential adherence—differences in whether trial participants took the antiretroviral drugs correctly. Antiretroviral drugs only control HIV infections effectively when they are taken regularly and adherence to antiretroviral PrEP is probably also important for HIV prevention. Here, the researchers investigate adherence to antiretroviral prophylaxis in a substudy within the Partners PrEP Study, a placebo-controlled RCT of oral antiretroviral drugs among nearly 5,000 HIV-uninfected members of serodiscordant couples in East Africa. In serodiscordant couples, only one partner is HIV-positive; 20% of couples in Africa who know their HIV status are serodiscordant. In the Partner PrEP Study, the efficacy of HIV protection with oral antiretroviral drugs was 67%–75%.
What Did the Researchers Do and Find?
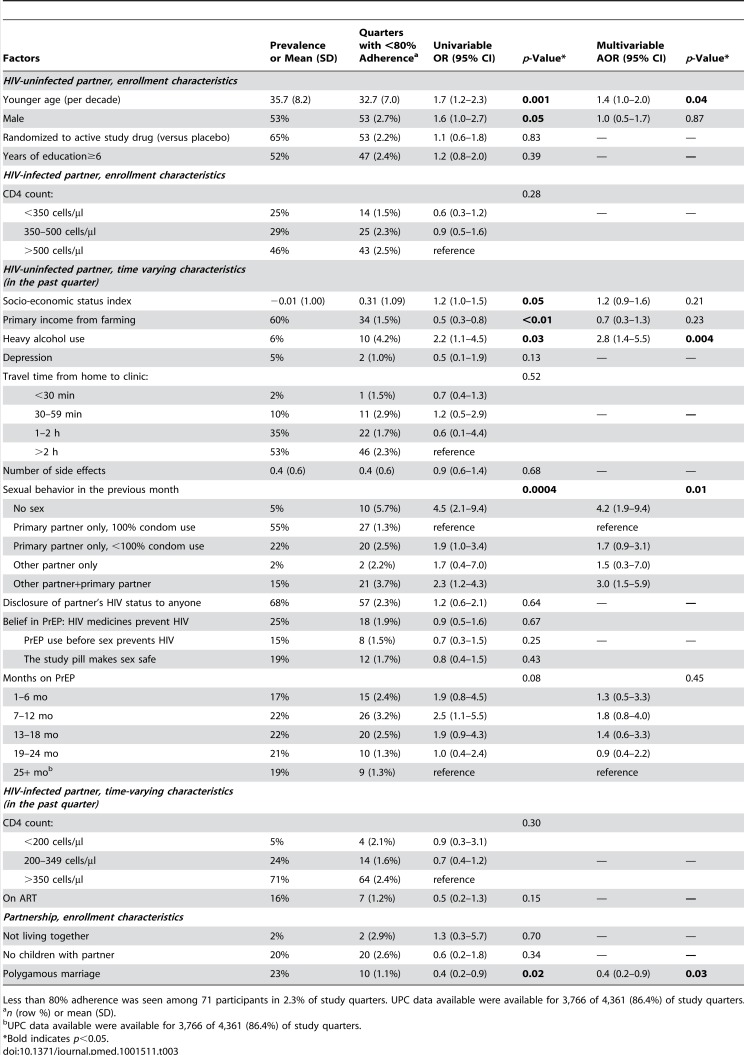
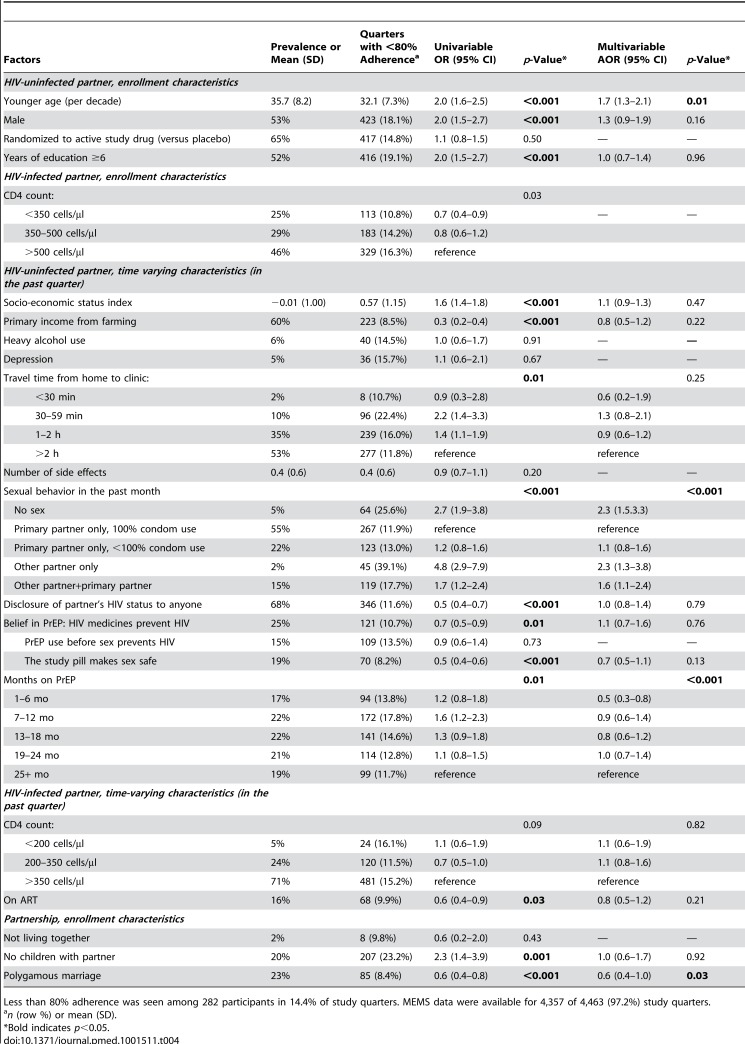
The researchers selected a “convenience” sample—a sample is taken non-randomly from a population that is close at hand—of 1,147 HIV-uninfected partners enrolled in Uganda. They used unannounced home-based pill counts (an approach that reduced the chance of participants dumping unused pills to appear more adherent than they actually were) and electronic pill bottle monitoring (a microchip in the medication bottle cap recorded whenever the bottle was opened) to measure PrEP adherence in this cohort. All the participants received adherence counseling at PrEP initiation and throughout the study; counseling was intensified if unannounced pill count adherence fell below 80%. Fourteen participants, all of whom had been assigned to placebo, became HIV-positive during the adherence substudy. The average adherence to PrEP was 99.1% and 97.2% as measured by unannounced pill counts and by electronic monitoring, respectively. About 7% and 26% of participants had less than 80% adherence as measured by unannounced pill count and electronic monitoring, respectively, during at least one 3-month period of the substudy. Greater than 80% adherence was associated with the first 6 months of PrEP use and polygamous marriage. Adherence less than 80% was associated with report of no sex or sex with another person besides the study partner, younger age, and heavy alcohol use. Finally, the adherence intervention (intensified counseling) was well received and in the first unannounced pill count after the intervention, adherence increased to above 80% in 92% of participants.
What Do These Findings Mean?
These findings indicate that the high level of PrEP adherence achieved in the setting of active adherence monitoring and counseling support was associated with a high level of protection from HIV acquisition by the HIV-uninfected partner in heterosexual serodiscordant couples. The findings also suggest that low PrEP adherence is associated with sexual behavior, alcohol use, younger age, and length of PrEP use. Several aspects of the study design may limit the accuracy of these findings. For example, although the adherence measures used here are probably more accurate than participant reports of missed doses and clinic-based pill counts (adherence measures that are often used in RCTs), they are not perfect. Nevertheless, these findings provide further support for the ability of PrEP to prevent HIV acquisition when taken regularly; they suggest that adherence interventions in the implementation setting should address sexual behavior, risk perception, and heavy alcohol use; and they provide data to guide ethical decisions about resource allocation for prevention and treatment of HIV infection.
Additional Information
Please access these Web sites via the online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001511.
-
Subjects:
-
Source:
-
Document Type:
-
Place as Subject:
-
Collection(s):
-
Main Document Checksum:
-
Download URL:
-
File Type:
-

gif 
jpeg 
gif 
jpeg 
txt 
gif 
jpeg
txt 
gif 
jpeg 
gif 
jpeg
 [PDF-270.27 KB]
[PDF-270.27 KB]
Details:
Supporting Files







More +


 Email
CDC-INFO
Email
CDC-INFO









